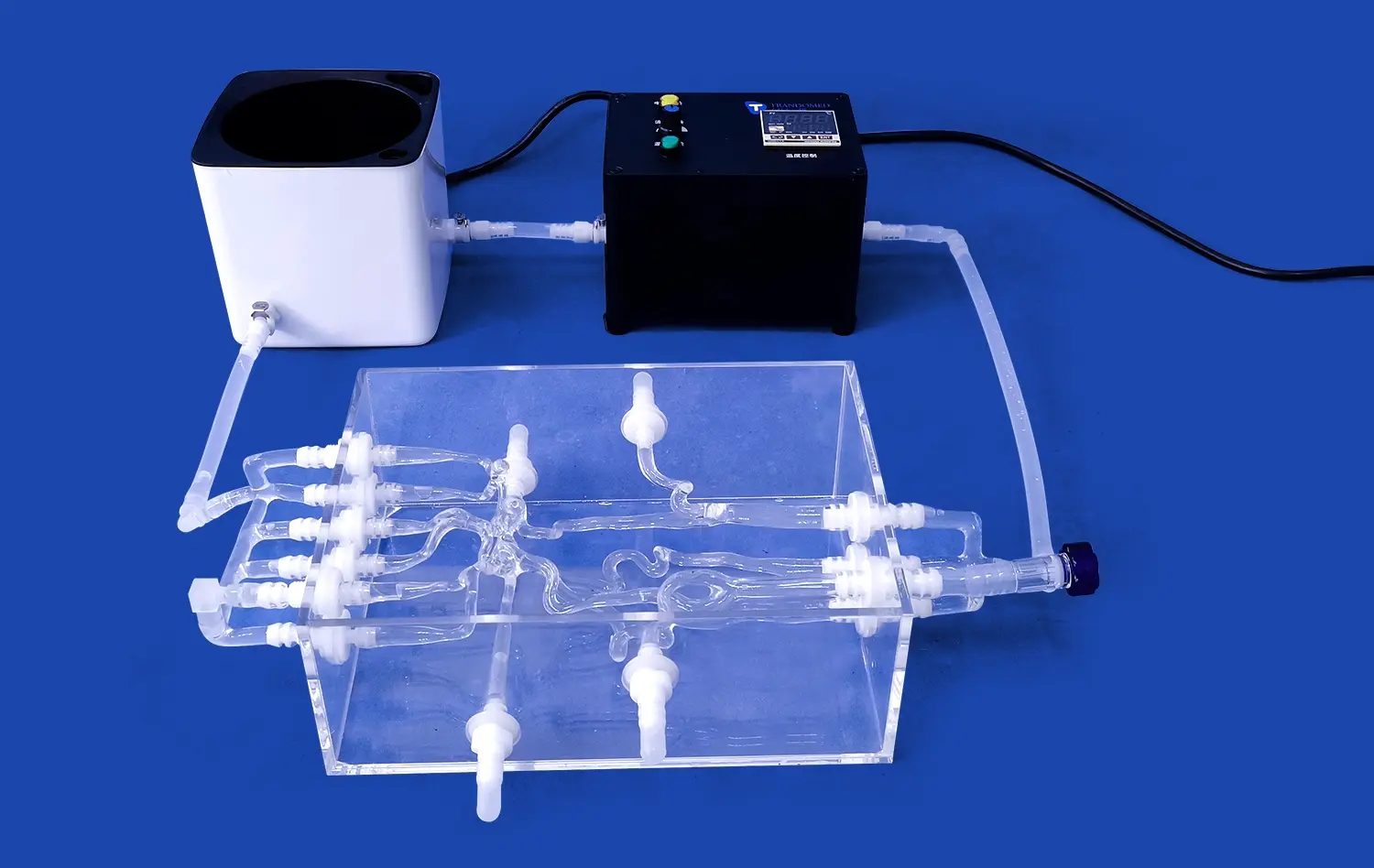
Advanced anatomy models made of plastic are changing how doctors learn and practice neuro-interventional treatments. A 3D artery model lets you see and feel complex brain structures, like the middle cerebral artery and internal carotid paths, in a way that is true to life. In contrast to standard two-dimensional images or corpse examples, these teaching aids allow for repeated, hands-on practice of catheter guidance, guidewire handling, and aneurysm treatment models. These precision-engineered models are being used more and more by medical schools, clinical training centers, and device makers to bridge the gap between theory knowledge and real-world procedural skill. This improves patient safety and therapeutic results in the long run.
Understanding 3D Artery Models in Neuro-Interventional Education
With the development of volumetric anatomy models, neuro-interventional training has changed in a big way. These specialized teaching tools give purchasing managers and clinical instructors a chance to see the anatomy of the cerebrovascular system in three dimensions that has never been seen before. Modern vascular models make artery networks that look like real patients' bodies more real and can be manipulated. Traditional training methods often rely on flat x-ray pictures or limited access to cadavers.
Differentiating Between Generic and Patient-Specific Models
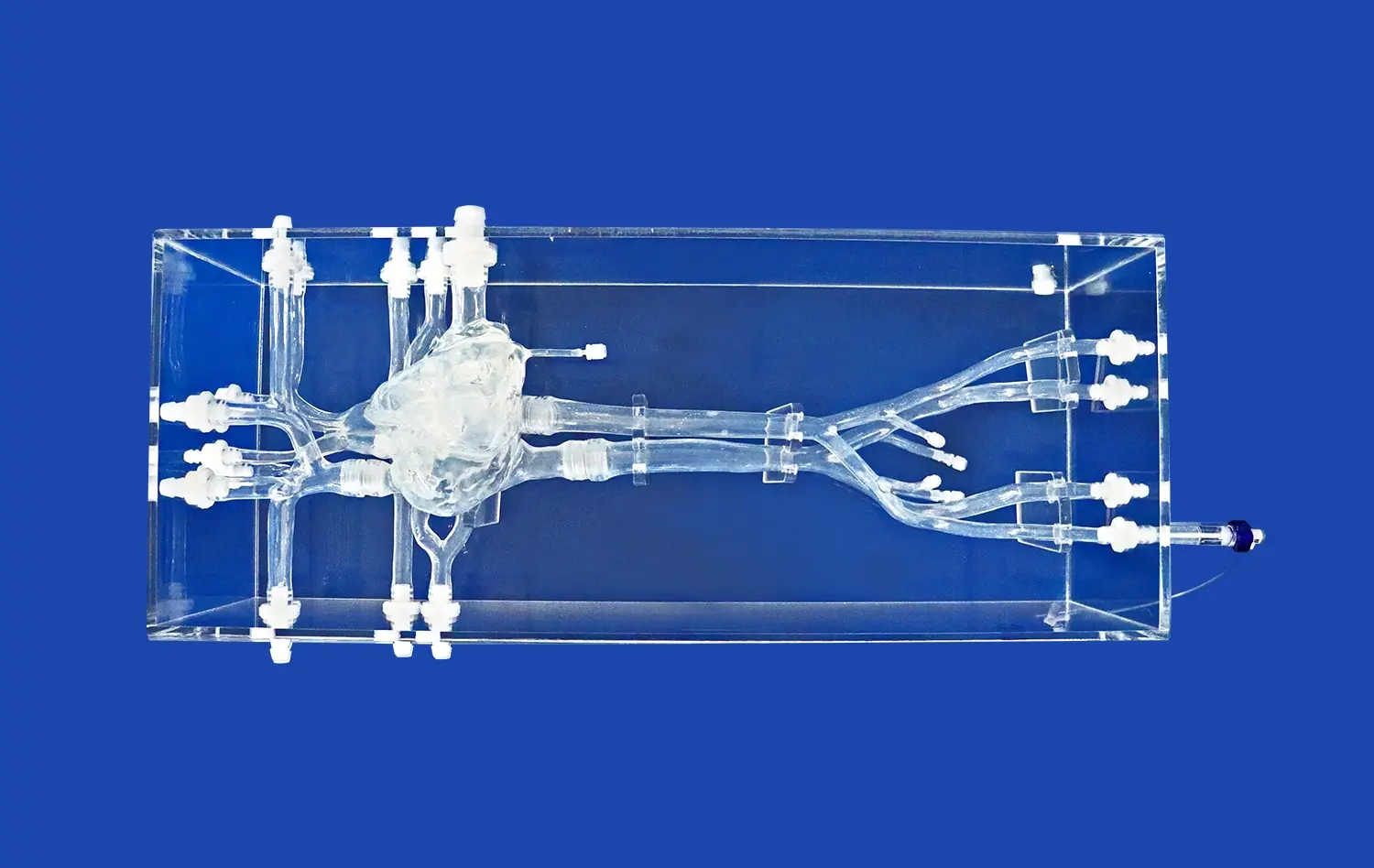
It is important to know the difference between regular and personalized anatomy models in order to make smart choices about what to buy. Generic arterial models accurately reflect the normal human cerebrovascular structure and are useful for building basic skills. The Circle of Willis, arterial bifurcations, and major brain veins are usually set up in normal ways in these models. Medical schools and nursing schools often use these uniform forms to teach big groups of students about basic anatomy connections and how to do catheterizations.
Patient-specific models represent a different category entirely. Because they are made from real CT angiography or MRI data, these personalized copies show differences in anatomy, diseases, and the way blood vessels are arranged in different people. More and more, hospitals getting ready for complicated neuroendovascular treatments use these custom tools to practice before the surgery. Interventional teams can prepare for problems, choose the right tools, and improve their technique before going into the operating room by practicing on a perfect copy of a patient's blood vessels.
Material Considerations and Durability Factors
The choice of material has a direct effect on both the teaching value and the useful life of arterial training models. Because of its physical qualities, Silicone Shore 40A is a great choice for simulating the cerebrovascular system. This particular durometer grade gives physical feedback that is very close to that of human artery tissue. This lets trainees develop realistic haptic awareness while manipulating catheters and putting devices in place.
Durability considerations extend beyond mere physical resilience. When you use high-quality silicone mixtures, they keep their shape after hundreds of workouts without breaking down much. Because they last so long, training schools can save a lot of money because one high-quality model can be used for many years. Silicone-based models are great for intense training programs because they don't tear easily, keep their shape after being manipulated many times, and work with standard medical devices.
Interpretation Techniques for Accurate Neurovascular Education
To get the most teaching value from anatomy models like the 3D artery model, they need to be properly integrated into organized lessons. The first step in good analysis is to connect the physical model to the imaging studies that go with it. Trainees learn how to mentally switch between how an angiogram looks and how the arteries really are built in three dimensions, which is a very important skill for real-life treatment. Teachers can help students learn more by showing digital subtraction angiography along with the real model at the same time. This will help students understand projection angles and vessel overlap.
For more advanced reading methods, these models are used to teach the reasoning behind choosing a catheter, optimizing the approach angle, and figuring out the right size for a device. Trainees learn how to use guide catheters through a fake middle cerebral artery by feeling their way through it. This helps them understand how vessels bend and how important it is to position the support catheter correctly. This hands-on experience builds trust in the steps that can't be achieved through computer models or learning by watching others.
Advantages of Using 3D Artery Models in Neuro-Interventional Training
There are some problems with traditional neurointerventional education that make it hard to get and lower the level of training. Access to cadavers is still very limited, and many schools can't provide enough bodies for their training programs. Even though virtual reality systems are very advanced technology, they don't have the real-life physical feedback that is needed to improve hand-eye coordination. These problems can be fixed with anatomical models made of medical-grade plastic, which also has other benefits that make learning better and the school run more smoothly.
Enhanced Learning Through Realistic Tactile Feedback
Describing or showing films of moving a microcatheter through a twisted vessel is not enough to fully capture the feeling. High-fidelity vascular models show real resistance patterns, which help trainees understand what to do when a device hits a curved vessel, a buildup of plaque, or an aneurysm neck. This training in the senses is very helpful for learning how to use a gentle touch during neuroendovascular treatments, since too much force can damage or puncture a blood vessel.
One more big benefit is that practice makes perfect. Anatomical models let you move from simple to complicated scenarios in a planned way, unlike patient cases, which can happen at any time and vary in how hard they are. Residents can practice the same steps over and over, getting better at them with each time. This way of conscious practice speeds up learning new skills and creates muscle memory for important tasks like placing stents and deploying coils.
Pre-Surgical Planning with Patient-Specific Models
Surgical teams getting ready for difficult aneurysm fixes or arteriovenous malformation treatments don't know a lot about how to do the procedures. These risks can be reduced by using patient-specific arterial models that let the whole procedure be practiced before the real surgery. In a risk-free setting, neurosurgeons can try out different pairings of catheters, check to see if an entry route is possible, and look for possible problems.
This training using a 3D artery model goes beyond just practicing the technical parts. When everyone on the team can see the biological task ahead of them, they can work together better. Interventionalists, anesthesiologists, and nurse staff work together to make sure everyone understands the steps of the procedure, the devices that are needed, and any problems that could happen. This kind of planning cuts down on the time needed for surgery, lowers the amount of radiation patients are exposed to, and eventually makes patients safer by making medical teams better prepared.
Cost Efficiency and Long-Term Investment Value
Even though the original costs of buying a good arterial simulator are something to think about, the overall cost of ownership is much lower than other ways to train. A strong plastic model can be used for hundreds of training sessions before it needs to be replaced. This spreads the cost of buying one over many students and practice sessions. The low cost is further increased by the fact that these types only need to be cleaned every so often with standard disinfectants.
Product testing and display uses give companies that make medical devices more value. Instead of using expensive prototypes on non-recoverable cadavers for testing, companies can use reused anatomical models to check the trackability of catheters, the flexibility of guidewires, and the way implants are deployed. When sales engineers have these display tools with them, they can effectively talk to possible customers about the benefits of the product, which leads to more productive discussions during hospital evaluations.
Key Applications of 3D Artery Models in Neuro-Interventional Education
Precision-engineered arterial models can be used in a wide range of training and professional settings. These tools have different but related uses in the medical environment. For example, research institutions train the next generation of interventionalists, and established hospitals make sure their staff is up-to-date on their skills.
Hands-On Simulation for Skill Acquisition
Neurosurgery residency programs have to work hard to make sure that residents get enough hands-on experience with procedures in the time they have available for training. Anatomical models get around this problem by adding organized training events to clinical case experience. Before doing these things on real patients, residents practice basic skills like choosing the right shape for a guide catheter, getting stable distal access, and handling catheter swaps.
Realistic arterial modeling such as the 3D artery model is also helpful for training in interventional radiology fellowships. Fellows get good at diagnostic cerebral angiography by doing selected catheterization of all the major blood channels inside the brain over and over again. Being able to make mistakes and learn from them without any negative consequences speeds up the learning process and keeps patients safe. Experts also use these models to keep their skills up when they don't have any complicated cases to work on or when they need to learn new ways to do things.
Enhancing Diagnostic Accuracy and Visualization
When neuroradiologists only use angiographic images to look at a patient, they often run into problems with complex vascular abnormalities. Three-dimensional physical models make it clearer how things relate to each other in space that aren't clear in two-dimensional images. It's easier to understand dural arteriovenous fistulas, which have complex networks of feeding arteries and draining veins, when you look at them in real life instead of trying to remember them from different angiographic views.
Anatomical models that are used in case talks are very helpful for educational conferences and meetings of diverse teams. Instead of looking at displayed pictures, doctors can use real copies to show disease, which makes talks about treatment options more in-depth. This better representation helps team members with less experience the most, because they can learn more about anatomy by looking directly at abnormal traits.
Integration into Academic and Corporate Training Programs
Neuroanatomy classes at medical schools are using simulations as a way to teach more and more. Students remember more about anatomy when they directly trace artery routes through silicone models instead of just reading textbooks and using digital tools. This hands-on method of learning works for a variety of learning styles and builds basic skills that are needed for higher clinical training.
Medical gadget firms know that trained users are what make products popular and work well in the office. Anatomical models are used in corporate training programs to teach doctors how to choose the right devices, how to use them correctly, and how to handle complications. When sales reps show that they really understand routine problems, they build technical confidence. They can do this by practicing with the same tools that their clinical customers use to improve their skills.
Conclusion
For better neurointerventional education and clinical readiness, realistic anatomy models such as the 3D artery model have become essential tools. The switch from old-fashioned training methods to advanced models made of silicone fixes long-standing problems in medical education and adds new features for individual learning and planning before surgery. When institutions buy good vascular models, they are at the cutting edge of training methods that are backed by evidence and have been shown to improve practical skills and patient results. As neuroendovascular methods keep getting better, physical, three-dimensional training tools will become even more important. This means that choosing the right provider will become more and more important for the success of the school.
FAQ
How long does it usually take to get custom-made brain models?
Standard customization jobs usually take seven to ten days from the time the final specs are approved until they are shipped. This schedule includes the process of verifying the design, making sure the model is perfectly made, and testing to make sure it meets all the requirements. We make it clear during the quote process if more time is needed for complex changes that involve very odd physical traits or multiple disease conditions. Depending on production plans, rush orders can sometimes be met. Institutions with important training targets should talk about their needs during the initial meetings.
How do training models made of plastic compare to models made from dead bodies?
Silicone-based anatomy models are better than cadaveric materials in a number of important ways. Tissue preservation changes the way corpse veins feel, making them either too stiff or too weak for realistic catheter practice. Silicone versions keep their physical qualities stable over time, so they can be used for hundreds of training sessions and still give accurate touch feedback. Also, plastic models don't have the logistics problems, moral issues, or biohazard worries that come with using real tissue samples. While cadavers are still useful for some parts of surgery education, high-fidelity models are much better for learning how to do procedures in therapeutic fields.
Can patient-specific models really make surgery go better?
There is a lot of proof that patient-specific procedure practice is helpful in the office. Studies that look at pre-surgery modeling show that when surgical teams practice on physically accurate models before treating real patients, they have shorter operating times, fewer complications, and more successful procedures. Teams can find the best ways to do things and plan for problems by testing different device choices, access routes, and rollout methods ahead of time. This planning is especially helpful in difficult cases with odd anatomy or high-risk disease, where not knowing how to do something can have big effects on the patient's health.
What kinds of upkeep do arterial training models need?
To make their total cost of ownership more appealing, high-quality plastic models don't need much upkeep. Cleaning regularly with light soap and water gets rid of any leftover contrast media or procedure waste. Regular checks for wear, especially at high-stress areas like tight vessel bends, help figure out when replacement is needed. Proper keeping away from direct sunlight and high temperatures keeps the qualities of things for a long time. Unlike electrical simulations that need to have their software updated, their calibrations changed, or parts replaced, anatomical models don't need any upkeep for as long as they're working, which is usually measured in years instead of months.
Partner with a Leading 3D Artery Model Manufacturer for Your Training Needs
Trandomed wants medical facilities, gadget makers, and study groups to look into how our physical modeling solutions can improve your treatment results and training programs. No matter if you need standard models to teach basic skills or patient-specific copies to plan complicated procedures, our engineering team is ready to talk about your needs. With more than twenty years of experience in medical 3D printing and skeletal modeling, we bring unmatched knowledge to every job, making sure that your money is well spent on education.
We welcome questions from sourcing professionals looking for dependable 3D artery model providers who can handle both one-time sales and long-term partnerships. Our promise of customization without design fees and quick production times of seven to ten days meet the needs of medical education programs that are always on the go. The ability to place bulk orders guarantees uniform quality, whether you need a single display unit or a full training lab set up.
Get in touch with jackson.chen@trandomed.com right away to get full product details, competitive quotes, and customized suggestions based on your institution's goals.
References
Anderson, J.R., Thompson, W.L., Alkattan, A.K., Diaz, O., Klucznik, R., Zhang, Y.J., Britz, G.W., Grossman, R.G., and Karmonik, C. (2016). "Three-dimensional printing of anatomically accurate, patient specific intracranial aneurysm models." Journal of NeuroInterventional Surgery, 8(5), 517-520.
Mashiko, T., Otani, K., Kawano, R., Konno, T., Kaneko, N., Ito, Y., and Watanabe, E. (2015). "Development of three-dimensional hollow elastic model for cerebral aneurysm clipping simulation enabling rapid and low cost prototyping." World Neurosurgery, 83(3), 351-361.
Ryan, J.R., Almefty, K.K., Nakaji, P., and Frakes, D.H. (2016). "Cerebral aneurysm clipping surgery simulation using patient-specific 3D printing and silicone casting." World Neurosurgery, 88, 175-181.
Stefaniak, P., Walocha, J.A., Klasterczyk, J., and Radomski, D. (2019). "Three-dimensional printing in interventional radiology: Current applications and future perspectives." Polish Journal of Radiology, 84, 245-251.
Torres, I.O., De Luccia, N., Calderaro, D., and Evangelista, F.H. (2017). "Simulation based training in vascular surgery: Educational assessment and improvement of clinical performance." Journal of Vascular Surgery, 65(3), 878-886.
Waran, V., Narayanan, V., Karuppiah, R., Owen, S.L., and Aziz, T. (2014). "Utility of multimaterial 3D printers in creating models with pathological entities to enhance the training experience of neurosurgeons." Journal of Neurosurgery, 120(2), 489-492.
_1736215128474.webp)
_1734507205192.webp)
_1732863962417.webp)