Through realistic training environments, advanced cardiac electrophysiology simulation is a game-changing way to learn and treat complex arrhythmias. The venous cardiac electrophysiology model is at the heart of this new idea. It mimics the heart's electrical pathways, focusing on venous structures such as the superior vena cava, inferior vena cava, and right atrial connections. These high-fidelity models let doctors practice catheter navigation, ablation procedures, and diagnostic mapping without any risk. This closes the gap between what they know in theory and what they can do in practice, and it also makes patients safer.
Understanding Venous Cardiac Electrophysiology Models
The Foundation of Cardiac Electrical Simulation
Cardiac electrophysiology studies the heart's complex system of electrical signals that control each beat. Traditional ways of teaching focused on dissecting bodies and two-dimensional pictures, which didn't always show how electrical conduction changes over time. Modern simulation models get around these problems by including physically accurate venous pathways that affect how arrhythmias start and spread.
A lot of normal learning materials don't talk about how important the venous system is to cardiac electrophysiology. Structures like the superior and inferior vena cava not only carry blood, but they can also send out electrical messages that aren't supposed to be there. Doctors can better understand how arrhythmias like atrial fibrillation start and persist when they use simulation models that correctly represent these venous components. This is especially true when pulmonary vein activity or right atrial dysfunction sets them off.
Technical Construction and Material Science
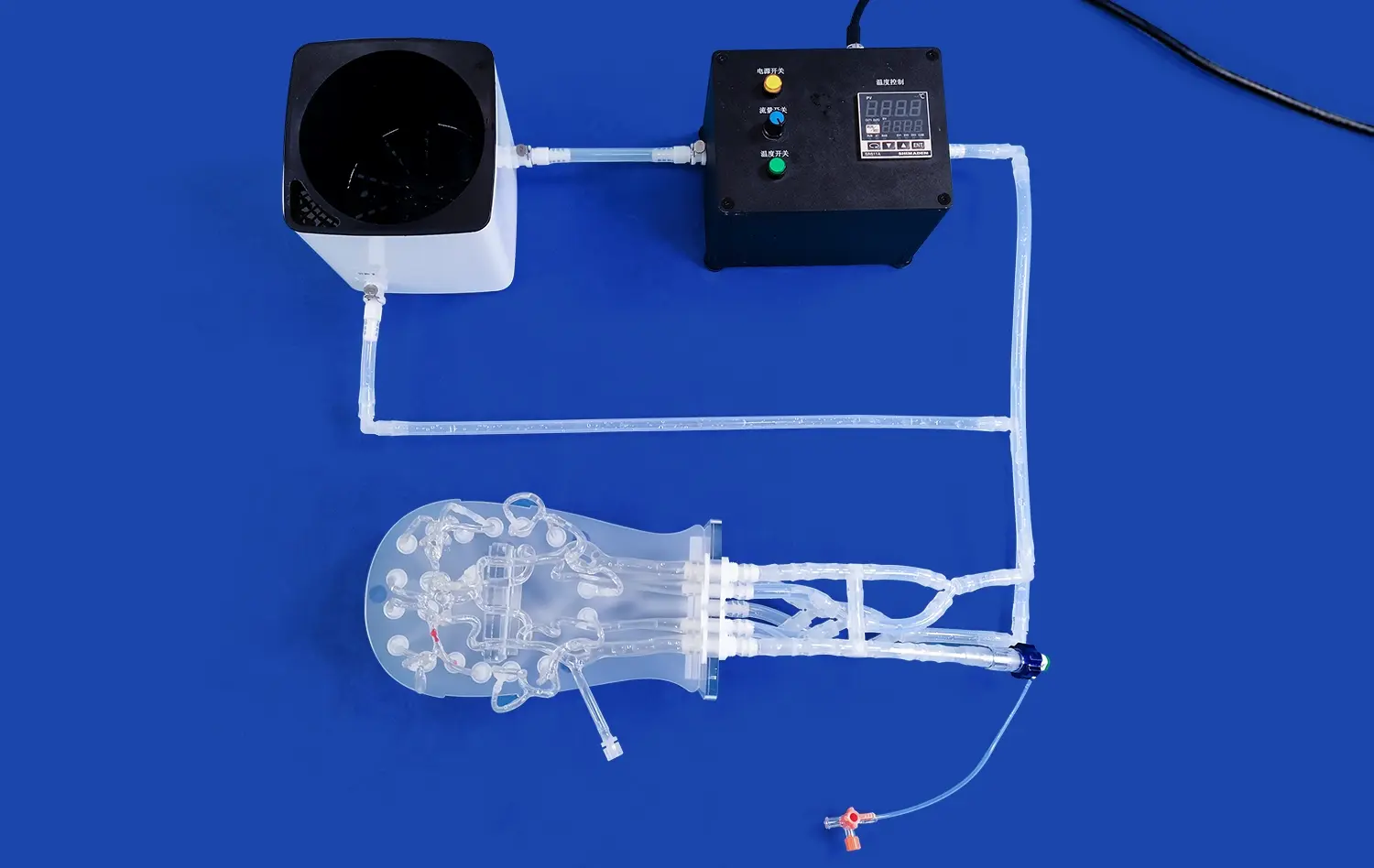
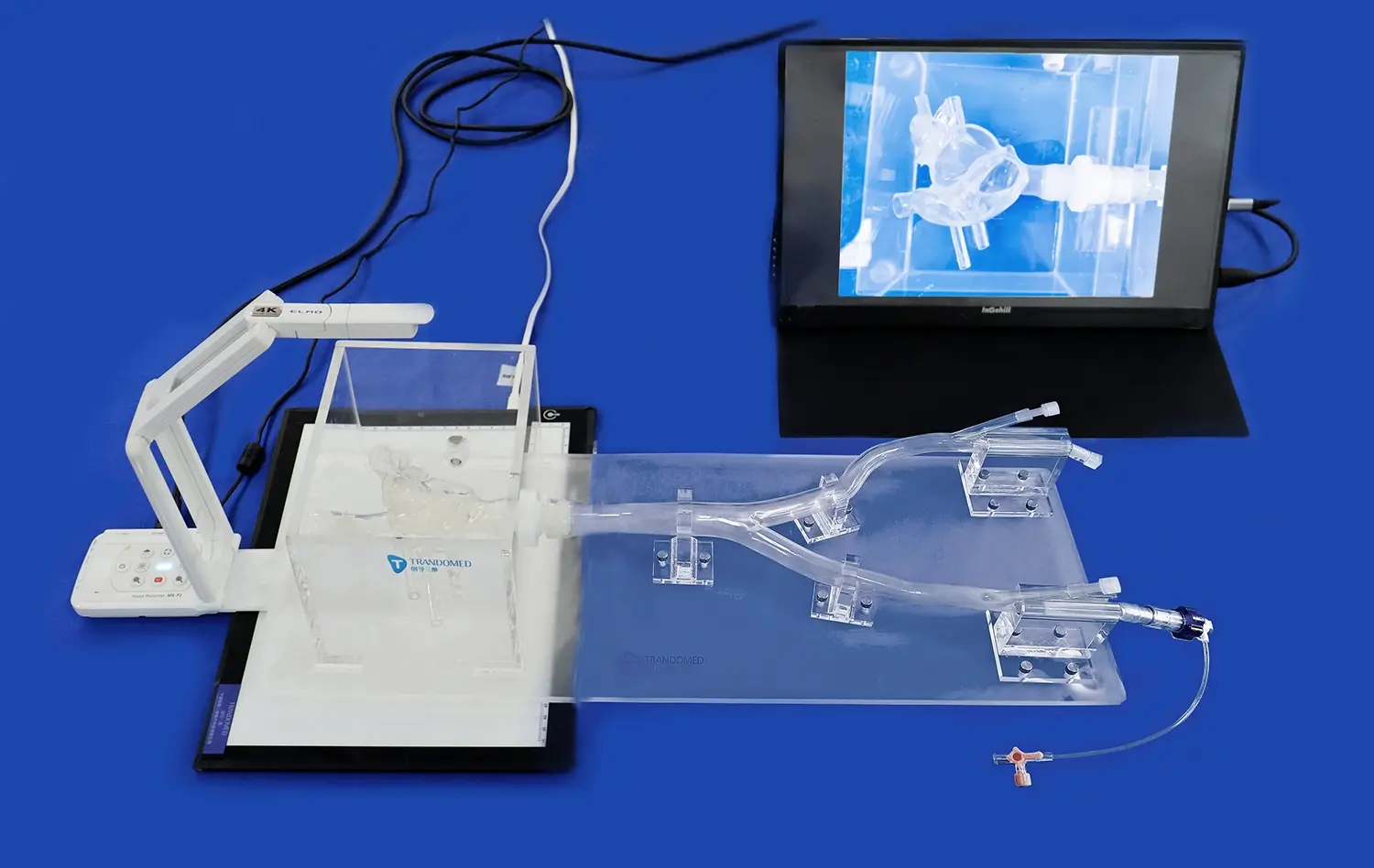
Medical-grade silicone materials are used in advanced simulation models because they are very good at mimicking the properties of human flesh. When manipulating a catheter, the Shore 40A silicone specification gives the best mix of durability and realistic tactile feedback. This choice of materials makes sure that doctors experience the real resistance and navigation problems they will face during real procedures. This means that training classes can really be used in real life.
The way these models are made has changed a lot since three-dimensional printing came along. Manufacturers can make anatomically variable models that reflect the variety seen in clinical groups by using CT and MRI scans of real patients. This method of reverse engineering finds small changes in structures that affect the success rate of procedures. It exposes trainees to both common and difficult changes in anatomy before they see them in the catheterization laboratory.
Physiological Principles Behind Venous Modeling
Understanding the two-domain model of cardiac electrophysiology gives designers of simulations a scientific base for their work. This computer model shows how electrical signals move through heart muscle, taking into account both the electrical fields inside and outside of cells. This model shows how the thin-walled atria and big venous tributaries create special electrical environments where arrhythmias can keep going with the help of reentrant circuits when it is applied to venous structures.
The right heart and the veins that connect to it are particularly difficult to study electrically. A muscle ridge in the right atrium called the crista terminalis acts as a natural electrical barrier that can break up transmission patterns. With these anatomical details included in simulation models, doctors can guess where ablation lesions should be put and figure out why some arrhythmias are hard to stop with standard methods.
Comparing Venous Cardiac Electrophysiology Models with Other Approaches
Physical Models Versus Digital Simulation
There are real benefits to using physical anatomical models instead of only digital simulation tools. When doctors move catheters through silicone anatomy, the tactile feedback they get builds muscle memory that directly affects their trust during the procedure. Computer-based simulators use force-feedback devices to simulate how tissues interact. Physical models, on the other hand, provide real resistance, friction, and navigation cues that help students remember what they've learned and improve their skills.
But computational models are useful in addition because they let us see electrical activity that we can't see during physical processes. Activation maps, voltage gradients, and propagation patterns can be shown on top of three-dimensional anatomy on software systems. It is best to train in a place that has both physical models for practicing skills and digital tools for understanding concepts. This way, students can get a full education that covers both the technical and mental sides of electrophysiology.
Venous Models Versus Arterial Approaches
Because interventional cardiology has been so important in the past, traditional cardiac modeling often focuses on artery access and coronary intervention. When we look at venous electrophysiology models, they focus on the right heart chambers and systemic venous branches, which is where most arrhythmia treatments happen. This difference is important because venous navigation is different from arterial catheterization in a number of ways, such as the need to be able to handle thinner artery walls, deal with tricky angles at the junction of the superior vena cava and the atrial septum, and know how the tricuspid valve works.
There are also big differences between the clinical uses. Arterial models help doctors learn how to do coronary angiography and stent placement, and venous models help them learn how to put in pacemakers, do electrophysiology studies, and do catheter ablation techniques. Both types of models are useful for medical facilities that treat a wide range of patients, but programs that focus on electrophysiology get more out of buying high-quality venous simulation systems that match their clinical priorities and training goals.
Comparing Standard ECG Analysis with EP Studies
Electrocardiograms are useful for screening, but they don't have the spatial resolution or diagnostic accuracy of electrophysiology tests. EP studies use intracardiac catheters to record signals straight from the heart chambers, while ECG tracings show electrical activity from the outside of the body. This difference is like comparing pictures taken by satellites of the weather with readings made on the ground. Both are useful, but they do different things and aren't as accurate.
This conceptual gap is filled by simulation venous cardiac electrophysiology models that let students connect results from surface ECGs with those from intracardiac electrograms. Trainees can move catheters through a model of the body while watching how different angles produce different electrical signals. This helps them make mental maps that connect patterns on the surface to places in the body. When doctors have to read complicated electrical data in real time while moving diagnostic and ablation catheters, this all-around understanding comes in very handy.
Applications and Benefits of Venous Cardiac Electrophysiology Simulation
Clinical Training and Skill Development
Medical schools and residency programs are always under fire to make training more efficient while keeping patients safe. This problem can be solved by simulation-based education, which gives students endless chances to practice without putting patients at risk. Trainees can do treatments over and over until they get good at them. They can also make mistakes that would be dangerous in a clinical setting and get feedback right away on their technique and decision-making.
In the past, electrophysiology procedures needed a lot of patient exposure as a way to learn them. This created ethical problems between the education of trainees and the care of patients. This learning curve is sped up a lot by high-fidelity computer models. Studies show that doctors who are taught on realistic models reach competency standards a lot faster than doctors who only use traditional apprenticeship methods. This is good for both the learners and the patients they will eventually treat on their own.
Preoperative Planning and Complex Case Preparation
In addition to teaching basic skills, patient-specific models made from CT or MRI pictures allow for personalized planning of procedures. Before going into the electrophysiology laboratory, doctors can practice difficult ablation treatments on models of their real patients' bodies. This helps them figure out the best ways to use catheters and prepare for technical problems. During fluoroscopy-guided interventions, this preparation cuts down on process times, raises success rates, and lowers the amount of radiation patients are exposed to.
Differences in anatomy have a big effect on how hard and how often complications happen during surgery. Patients who were born with heart disease, have had surgery in the past, or have unusually shaped veins can be especially difficult. Custom simulation models let electrophysiology teams come up with detailed plans for procedures, talk about different ways to do things, and make sure that everyone on the team knows what to do in important situations. By planning ahead, complicated situations are turned into well-rehearsed steps with backup plans ready in case something goes wrong.
Device Testing and Product Development
Anatomical models are used by companies that make medical devices all the way through the product development process. During the design process, engineers test prototypes on real bodies to find problems with how they work before they go through expensive clinical trials. For product demos, marketing teams use these models, which show off the features of devices better than simple text or two-dimensional diagrams.
For more and more regulatory approvals, bench testing data showing how well the device works in anatomically related models is needed. High-quality simulation systems offer standardized testing grounds that produce repeatable data that helps with FDA submissions and applications to foreign regulatory bodies. Investing in high-quality anatomical models pays off in the form of shorter development times and stronger regulatory documentation that can stand up to close review during the approval process.
Research Applications and Innovation
Biomedical research labs use electrophysiology models to look into how arrhythmias work, try out new ablation methods, and make sure that computer estimates were right. These models give scientists controlled test settings where they can focus on certain body parts and change them in a planned way. Researchers can change the model's features to see how changes in structure affect electrical conduction. This gives us basic information that helps us understand both in theory and in real practice.
Physical models that connect basic science finds to clinical applications are especially helpful for translational medicine projects. When lab results point to a new way to treat a condition, trying its viability on realistic body models is very important to get proof-of-concept data before starting studies on humans. By doing this intermediate validation step, resources are saved, patient safety is protected, and the chances of good basic research leading to better treatments are raised.
How to Choose and Procure Venous Cardiac Electrophysiology Modeling Solutions?
Essential Evaluation Criteria
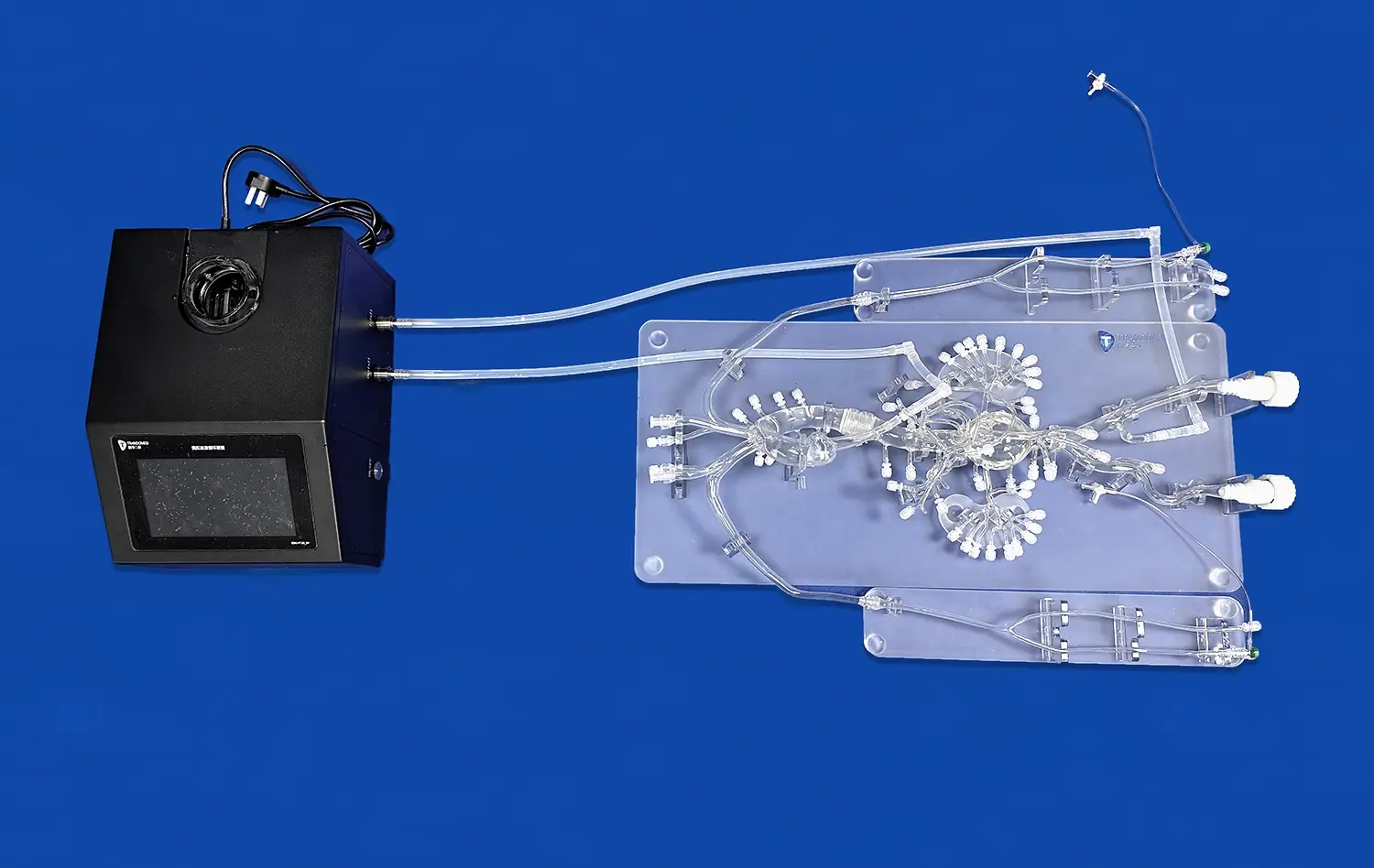
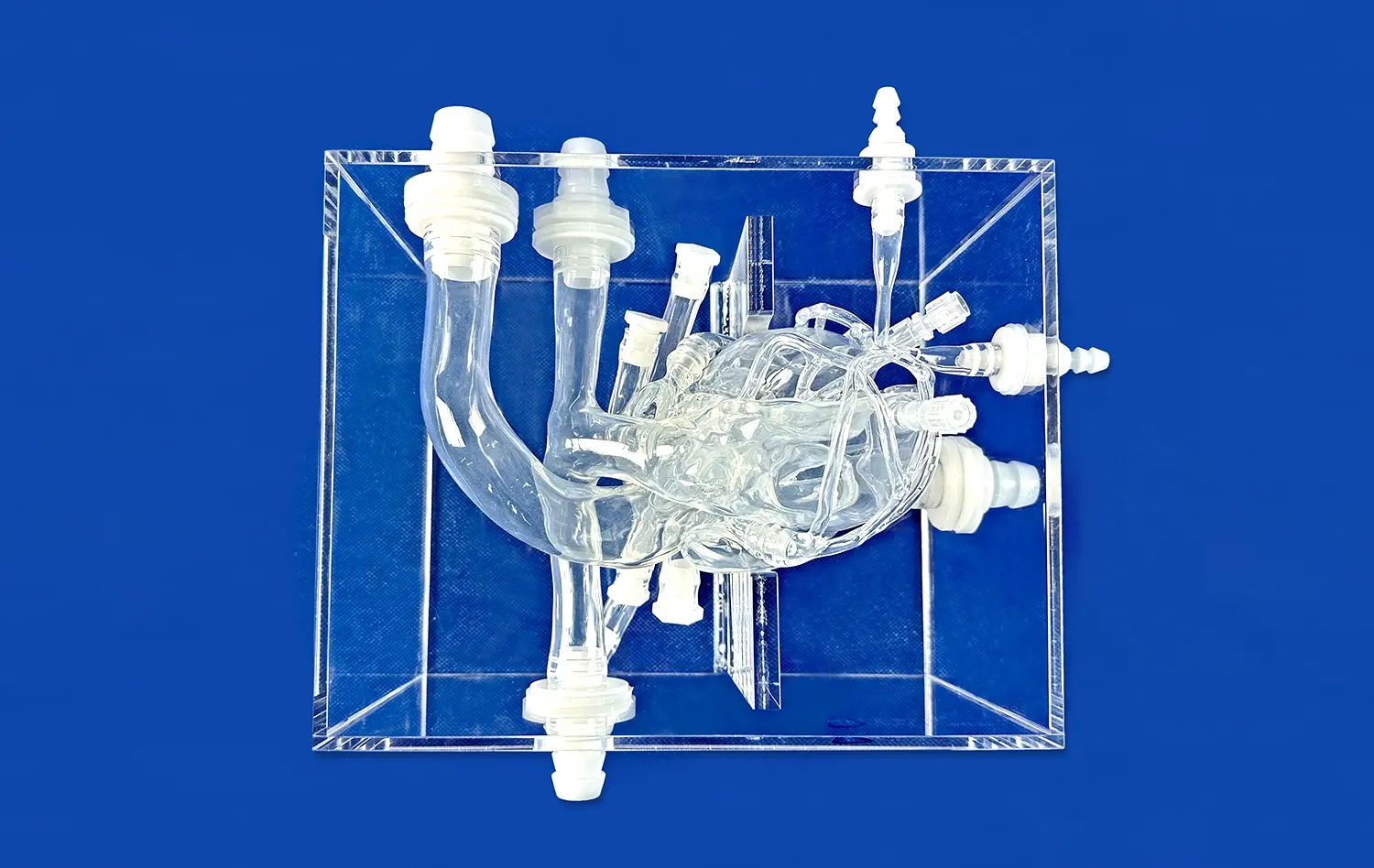
Selecting appropriate simulation equipment requires careful assessment of several technical specifications. Anatomical accuracy stands paramount—models must faithfully reproduce structures relevant to intended training objectives. The Venous Cardiac Electrophysiology Model (XXS004) exemplifies this principle by incorporating the inferior vena cava, right atrium, right ventricle, superior vena cava, and subclavian vein with precise dimensional relationships that reflect actual human anatomy derived from extensive medical imaging databases.
Material properties significantly influence training effectiveness. Shore 40A silicone provides tissue-mimicking characteristics that facilitate realistic catheter manipulation, offering appropriate resistance during advancement and stability during ablation simulation. Durability matters equally, as training models must withstand repeated use without degrading or losing anatomical fidelity. Institutions should evaluate expected model lifespans and replacement costs when calculating total ownership expenses over multiyear training programs.
Customization Capabilities and Institutional Needs
Standard anatomical models serve many educational purposes, but advanced training programs often require customized solutions reflecting specific patient populations or research questions. Leading manufacturers accept CT, CAD, STL, STP, and STEP file formats, enabling creation of patient-specific replicas or anatomically variant models. The ability to adjust features like foramen ovale dimensions or reconstruct atrial segments using actual patient data transforms simulation from generic training into personalized procedural rehearsal.
Customization extends beyond individual models to comprehensive training curricula. Institutions should seek suppliers offering consultative relationships where engineers understand clinical workflows and educational objectives. This collaboration ensures delivered products genuinely support program goals rather than forcing training approaches to accommodate equipment limitations. The absence of design fees for customization, as offered by established manufacturers, removes financial barriers to obtaining ideally configured simulation tools.
Vendor Selection and Partnership Considerations
The simulation equipment market includes numerous suppliers with varying expertise levels. Procurement teams should prioritize manufacturers with substantial experience in medical 3D printing and documented understanding of cardiac electrophysiology. Trandomed brings over two decades of specialized focus to this field, translating clinical insights into simulation products that meet the exacting standards of electrophysiology training programs and research institutions worldwide.
Technical support and training services separate premium suppliers from basic equipment vendors. Effective simulation programs require ongoing assistance with model maintenance, usage optimization, and curriculum development. Manufacturers offering comprehensive support packages ensure institutions maximize their equipment investments through proper utilization and staff competency development. Evaluating vendor responsiveness, technical expertise, and commitment to long-term partnerships should weigh heavily in procurement decisions.
Financial Considerations and Investment Value
While acquisition costs represent obvious budget considerations, total cost of ownership provides more meaningful financial analysis. Durable models with longer usable lifespans justify higher initial investments compared to inexpensive alternatives requiring frequent replacement. Institutions should calculate per-trainee costs across expected equipment life to understand true economic value rather than focusing narrowly on purchase amounts.
The return on investment extends beyond direct training costs to include reduced complication rates, shorter procedure times, and improved first-case success rates among trained physicians. These clinical outcomes generate substantial institutional value through enhanced reputation, reduced liability exposure, and improved patient satisfaction scores. When viewed through this comprehensive lens, premium simulation equipment represents strategic investment in clinical excellence rather than discretionary educational expense.
Optimizing the Use of Venous Cardiac Electrophysiology Models in Practice
Integration into Training Curricula
Effective simulation programs integrate models systematically throughout educational progression rather than treating them as isolated training events. Beginning learners benefit from guided practice sessions focusing on basic catheter manipulation and anatomical orientation. Intermediate trainees progress to more complex scenarios involving arrhythmia diagnosis and ablation planning. Advanced practitioners use models for rare case preparation and technique refinement, ensuring skills remain sharp between clinical cases.
Curriculum designers should establish clear competency benchmarks tied to simulation performance metrics. Tracking parameters like procedure completion time, fluoroscopy duration, and complication avoidance creates objective assessment data supporting advancement decisions. This structured approach transforms simulation from subjective practice opportunity into rigorous competency validation that programs can document for accreditation bodies and quality assurance purposes.
Data Management and Performance Analysis
Modern training programs increasingly incorporate performance analytics that track trainee progress across multiple simulation sessions. Recording parameters like catheter path efficiency, contact force consistency, and anatomical recognition accuracy generates longitudinal data revealing learning trajectories and identifying struggling trainees requiring additional support. This evidence-based approach optimizes educational resource allocation while ensuring all program graduates achieve consistent competency standards.
Integration with institutional learning management systems streamlines data collection and analysis. Exporting simulation performance metrics alongside traditional didactic assessments creates comprehensive learner portfolios that inform personalized educational planning. Program directors gain visibility into curriculum effectiveness, identifying content areas where additional resources improve outcomes and justifying continued investment in simulation infrastructure through demonstrated educational impact.
Maintenance and Longevity Maximization
Proper model care significantly extends usable lifespan and preserves training effectiveness. Institutions should establish cleaning protocols appropriate to silicone materials, avoiding harsh chemicals that degrade surface properties or alter mechanical characteristics. Storage conditions matter equally—models maintained in temperature-controlled environments away from direct sunlight retain anatomical accuracy and material properties far longer than those stored haphazardly.
Developing institutional expertise in venous cardiac electrophysiology model maintenance reduces reliance on external service providers and minimizes equipment downtime. Designating trained staff members as simulation equipment coordinators creates accountability for proper care while ensuring someone can troubleshoot minor issues without manufacturer intervention. This operational approach maximizes equipment availability for training sessions while controlling long-term maintenance expenses.
Staying Current with Evolving Technology
Cardiac electrophysiology continues advancing rapidly, with new ablation technologies, diagnostic approaches, and anatomical insights emerging regularly. Simulation programs must evolve correspondingly to remain relevant. Maintaining relationships with equipment manufacturers who actively research and develop updated models ensures institutions can refresh their simulation inventories periodically, exposing trainees to current best practices rather than outdated techniques.
Professional development for simulation program staff parallels trainee education in importance. Faculty members who understand latest clinical evidence and procedural innovations design more effective simulation scenarios and provide more valuable feedback to learners. Attending electrophysiology conferences, participating in manufacturer training workshops, and collaborating with clinical colleagues keeps simulation educators aligned with frontline practice realities.
Conclusion
Advanced cardiac electrophysiology simulation transforms physician training through realistic models that replicate complex venous anatomy and procedural challenges. The integration of high-fidelity physical simulators with comprehensive educational curricula accelerates competency development while protecting patient safety during the learning process. As electrophysiology procedures grow increasingly sophisticated, simulation-based preparation becomes essential rather than supplementary to clinical education. Institutions investing in premium anatomical models, particularly those emphasizing venous cardiac structures, position their programs at the forefront of cardiovascular medicine training. The demonstrated benefits across clinical skill development, research applications, and device innovation justify viewing simulation equipment as strategic infrastructure supporting institutional excellence and improved patient outcomes across diverse healthcare settings.
FAQ
What distinguishes venous cardiac electrophysiology models from arterial-focused simulators?
Venous models concentrate on right heart anatomy and systemic venous structures where most electrophysiology procedures occur, including the superior vena cava, inferior vena cava, right atrium, and coronary sinus. Arterial models emphasize left heart structures and coronary circulation relevant to interventional cardiology. The procedural skills differ substantially—venous navigation requires managing thinner walls, different catheter behaviors, and understanding tricuspid valve relationships critical for pacemaker implantation and ablation procedures.
How does simulation complement traditional ECG diagnostics in electrophysiology training?
Surface electrocardiograms provide screening information but lack the spatial resolution that intracardiac mapping delivers. Simulation models allow trainees to correlate surface ECG patterns with specific anatomical locations by manipulating catheters while observing resulting electrical signals. This hands-on experience builds mental frameworks linking diagnostic findings to anatomical substrates, improving real-time interpretation skills during actual procedures when rapid decision-making proves essential.
What factors should procurement teams prioritize when purchasing cardiac electrophysiology models?
Anatomical accuracy derived from real patient imaging data ensures clinical relevance. Material properties must provide realistic tactile feedback—Shore 40A silicone offers ideal tissue-mimicking characteristics. Customization capabilities allow tailoring models to specific training needs or patient populations. Vendor experience in medical simulation and availability of ongoing technical support significantly impact long-term value and successful program implementation beyond initial equipment acquisition.
Partner with Trandomed for Superior Cardiac Simulation Solutions
Trandomed stands as a trusted venous cardiac electrophysiology model manufacturer specializing in 3D-printed anatomical simulators that elevate physician training and procedural outcomes. Our Venous Cardiac Electrophysiology Model (XXS004) delivers unmatched anatomical precision through silicone Shore 40A construction, incorporating the inferior vena cava, superior vena cava, right atrium, right ventricle, and subclavian vein with customization options at no additional design cost. Backed by over twenty years of medical 3D printing innovation and reverse reconstruction technology utilizing extensive CT and MRI databases, we provide solutions meeting the demanding standards of medical education institutions, hospitals, research laboratories, and device manufacturers across the United States. Our rapid 7-10 day lead times and flexible payment terms support urgent training needs. Connect with our team at jackson.chen@trandomed.com to discuss how our expertise can transform your cardiac electrophysiology training program through simulation tools designed specifically for clinical excellence and educational impact.
References
Josephson, M.E. (2016). Clinical Cardiac Electrophysiology: Techniques and Interpretations. Fifth Edition. Philadelphia: Wolters Kluwer.
Calkins, H., et al. (2017). HRS/EHRA/ECAS/APHRS/SOLAECE Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation. Heart Rhythm, 14(10), e275-e444.
Zipes, D.P. & Jalife, J. (2018). Cardiac Electrophysiology: From Cell to Bedside. Seventh Edition. Philadelphia: Elsevier.
Huang, S.K.S. & Wood, M.A. (2015). Catheter Ablation of Cardiac Arrhythmias. Third Edition. Philadelphia: Elsevier Saunders.
Natale, A. & Jalife, J. (2019). Interventional Cardiac Electrophysiology: A Multidisciplinary Approach. New York: McGraw-Hill Education.
Kligfield, P., et al. (2019). Recommendations for the Standardization and Interpretation of the Electrocardiogram: Part I-IV. Journal of the American College of Cardiology, 73(11), 1309-1345.
_1734507815464.webp)
1_1732869849284.webp)