Advanced Cardiovascular Simulation for Left Atrial Appendage Closure
2026-05-18 09:00:03
For people with atrial fibrillation, closing the left atrial appendage is a game-changing way to avoid strokes, but it takes a lot of practice to get good at this complicated procedure. With the help of specialized training models and advanced cardiovascular modeling technology, doctors can now improve their skills in a controlled, repeatable setting. A left atrial appendage closure simulator accurately mimics the heart's structure and how procedures work, so interventional cardiologists and electrophysiologists can practice important skills without putting patients at risk. It is now necessary for medical schools, hospitals, device makers, and research sites that want to improve patient outcomes and procedural competency to have these high-tech training tools.
Understanding Left Atrial Appendage Anatomy and Closure Procedures
The Role of the Left Atrial Appendage in Cardiovascular Health
The left atrial appendage is a small structure that sticks out from the left atrium of the heart and looks like an ear. This unique part of the heart's anatomy is very important for its regular function because it controls the volume inside the blood vessels by releasing natriuretic peptides when the heart's blood flow changes. The LAA is physiologically important, but it becomes clinically important in people with atrial fibrillation because blood pooling in this structure makes it a high-risk place for a clot to form. According to research, about 90% of the blood clots that lead to strokes in people with atrial fibrillation come from the LAA. This makes it an important area for treatment.
Clinical Indications for LAA Closure
By closing off the left atrial lobe, the risk of stroke that comes with atrial fibrillation is treated instead of the arrhythmia itself. This minimally invasive treatment helps people who are at a higher risk of having a stroke but can't take long-term anticoagulation therapy because it can cause bleeding problems, falls, or problems with how medications work together. The procedure includes blocking off the LAA to stop thrombi from forming. This is an alternative to taking blood thinners like warfarin, apixaban, rivaroxaban, or dabigatran for life. Clinical studies show that successfully closing the LAA leads to a large drop in the number of strokes that happen. This supports the use of this method as a central part of modern cardiovascular care.
Anatomical Variations That Challenge Procedural Success
Medical imaging studies have found four main LAA morphologies that have a big effect on planning procedures and choosing the right gadget. The chicken wing morphology shows up in about 48% of cases and is characterized by a unique bend in the structure of the appendage. The cactus type, which happens 30% of the time, has many lobes that point in different directions. In 19% of cases, the windsock configuration shows up as a single dominant lobe with a steady diameter. The cauliflower shape, which only happens 3% of the time, has complicated internal trabeculations and no main structure. Understanding these differences in anatomy is important for the success of the procedure. Realistic practice training is the best way to get the judgment and technical skills you need to work with different patient bodies.
Clinical and Educational Applications of LAAC Simulation Technology
Transforming Medical Education Through Risk-Free Practice
Simulation-based training has changed the way cardiovascular education is taught by letting medical students and working doctors practice over and over again without putting real patients at risk. In the past, training mostly involved watching others do things and not getting much hands-on practice during real procedures. This made it hard for trainees to learn and keep patients safe. Modern simulation platforms get rid of this problem by giving students unlimited practice chances where they can make mistakes, get feedback right away, and improve their skills in a safe setting. More and more, medical schools and nursing schools are using these tools in anatomy classes, procedural skills labs, and specialty training programs to help students get ready for clinical rounds by building their basic skills.
Pre-Operative Planning and Patient-Specific Rehearsal
Cardiovascular simulation models do more than just teach basic skills; they also help with complex planning before surgery, which directly improves the result of the procedure. From CT or MRI scan data, doctors can now make patient-specific models that let them practice difficult cases with anatomical clarity that matches the real patient they will treat. Before going into the procedure room, this personalized planning helps doctors think of problems that might come up, choose the best device sizes, plan catheter paths, and come up with backup plans. Studies that looked at surgical rehearsal show that using patient-specific simulation models during preparation can cut down on operative time, lower the risk of complications, and improve the success rate of the first try.
Certification and Competency Assessment Programs
Professional certification in interventional cardiology counts more and more on simulation-based testing to make sure that candidates are competent in procedures before letting them practice on their own. Major cardiovascular training centers have set up standard evaluation methods that use high-fidelity left atrial appendage closure simulators to measure technical performance, the quality of decisions, and how well people handle complications. In addition to standard evaluation methods, these assessment models offer clear and repeatable metrics that take away subjective biases from figuring out competency. Healthcare organizations benefit from this method because it makes sure that only properly trained professionals do these important processes. This protects patient safety and helps professionals grow.
Comparing Simulation Technologies: Selecting the Optimal Training Solution
Evaluating Fidelity Levels and Training Objectives
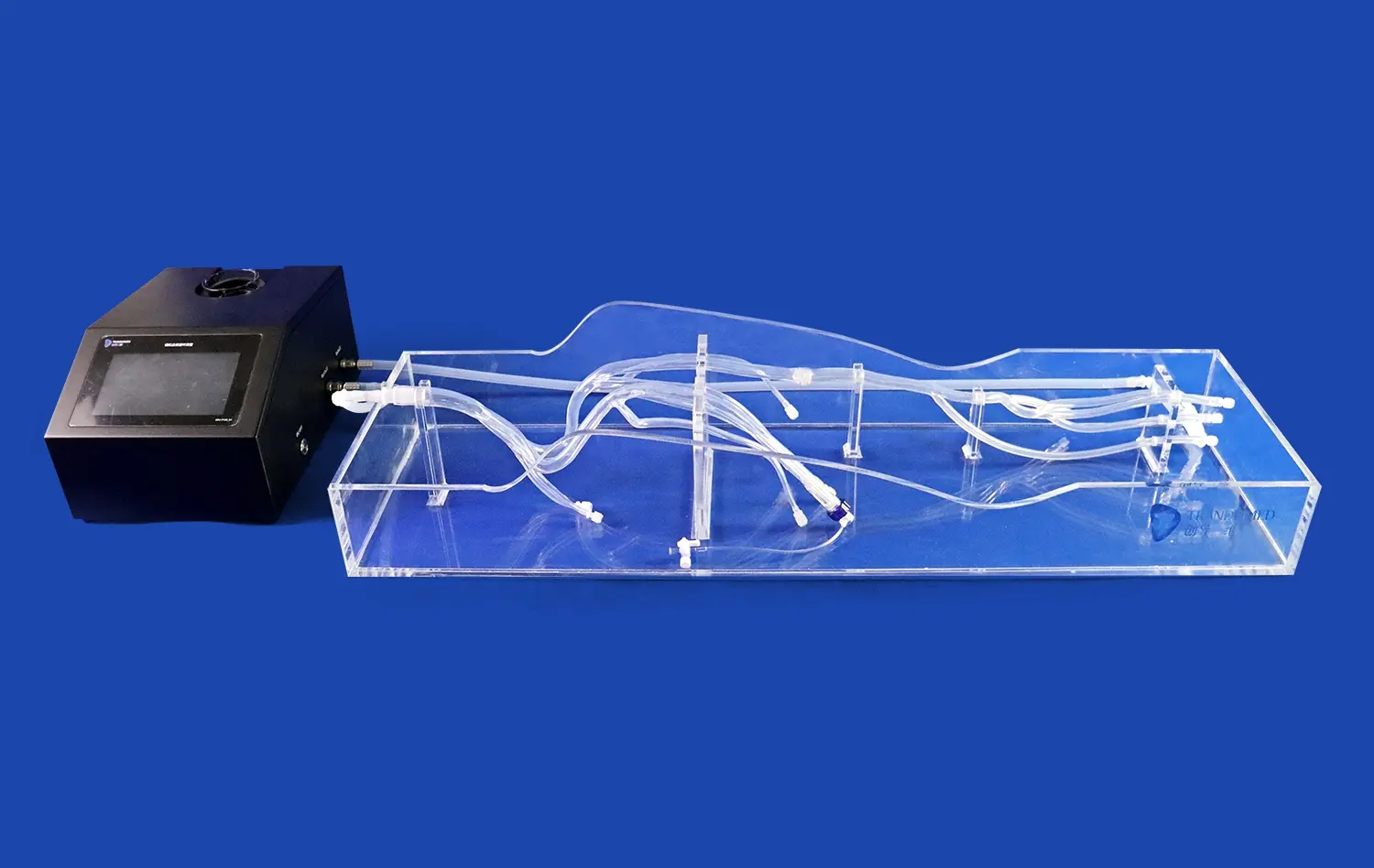
Simulation technology includes a wide range of levels of detail, from simple benchtop models to high-tech systems that can sense touch and have images built in. High-fidelity simulations have tactile feedback systems that very accurately model tissue resistance, catheter navigation forces, and device deployment dynamics. Most of the time, these high-tech platforms combine fluoroscopy simulation and echocardiographic visualization to make training situations that are very similar to real-life procedures. Lower-fidelity models are less realistic, but they are easier to move around with, last longer, and are easier for everyone to use. This makes them useful for learning basic skills and doing a lot of training.
Companies need to make sure that the simulators they choose are right for their training goals and the people they want to train. To support big student bodies, medical schools that focus on teaching procedural ideas may put an emphasis on being cost-effective and long-lasting. On the other hand, hospital training departments that are getting fellows ready to work alone need the highest levels of fidelity to make sure that skills can be transferred to clinical situations. When device makers show off their products, they need anatomically correct models that show off their technologies well. By understanding these different use cases, procurement choices can be made that lead to solutions that give the best return on investment.
Technical Specifications That Drive Training Effectiveness
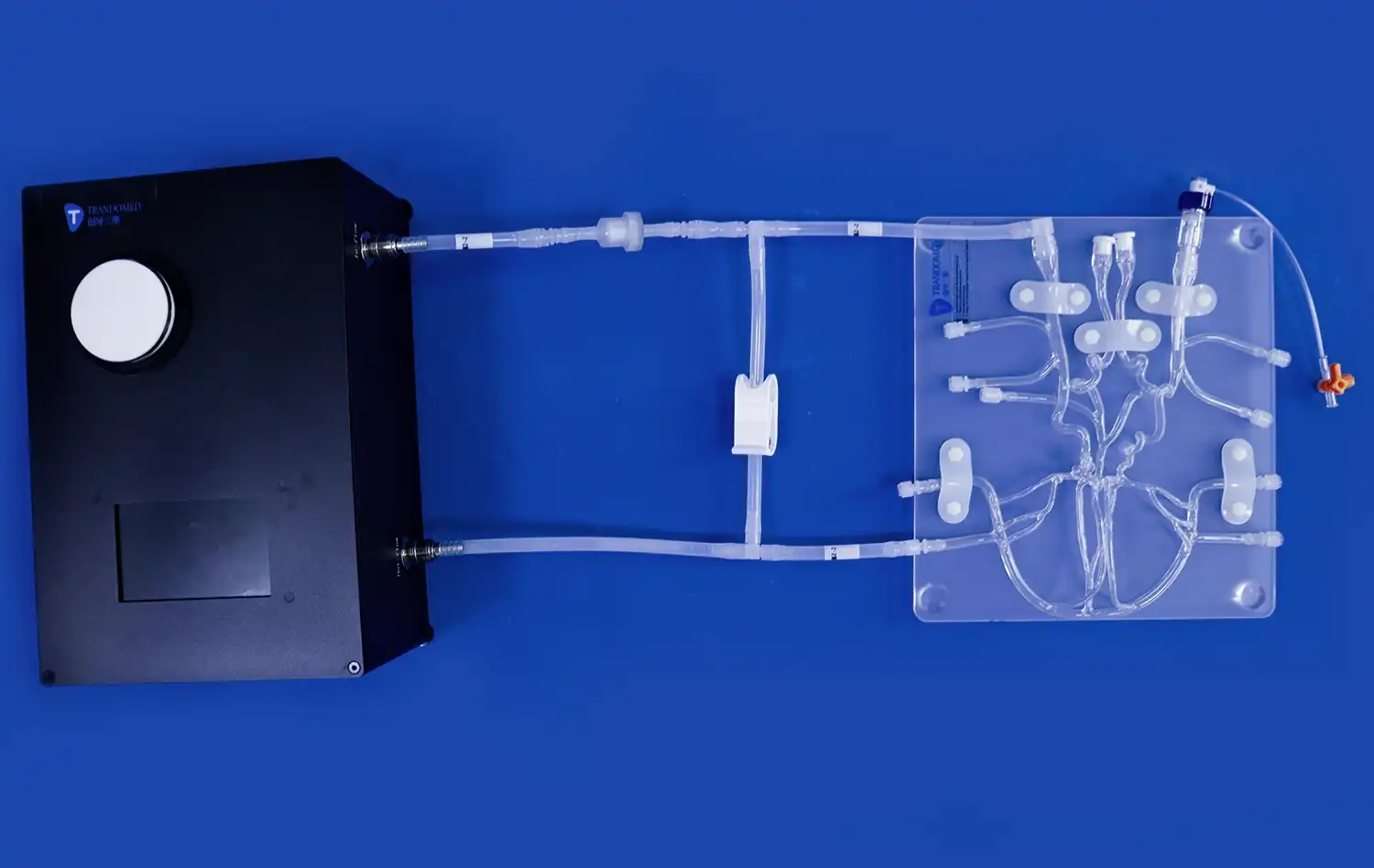
Anatomical accuracy, material qualities, modular design capabilities, and imaging compatibility are some of the most important technical factors to think about. The best training models accurately copy the heart and lungs by using a lot of human image data to get accurate measurements. The choice of material has a big effect on how realistic the feel is. Medical-grade silicones offer tissue-like flexibility and sturdiness that lasts through multiple training sessions. Multiple LAA shapes and different body types can be accommodated by modular designs. This gives trainers more options and makes simulation investments last longer. Standard fluoroscopy and echocardiography equipment compatibility makes sure that the system can be easily added to current clinical settings without needing to buy new infrastructure.
Return on Investment Considerations for Healthcare Organizations
When you do a financial analysis of simulation investments, you need to look at both the direct costs and the benefits to the company as a whole. Direct costs include buying the equipment in the first place, keeping it in good shape, replacing worn-out parts, and paying for program licenses. Traditional ways of training involve using animal models, cadaveric specimens, or long clinical apprenticeships, all of which come with ethical issues, the need to follow rules, and scheduling problems. These real costs are much better. Indirect benefits include fewer problems during procedures because operators are more skilled, shorter operating times because skills improve more quickly, easier hiring and keeping of top clinical talent drawn to schools with advanced training resources, and more procedures as more practitioners become skilled.
The Trandomed XX013D: Advanced Simulation for LAA Closure Training
Comprehensive Anatomical Replication and Modular Versatility
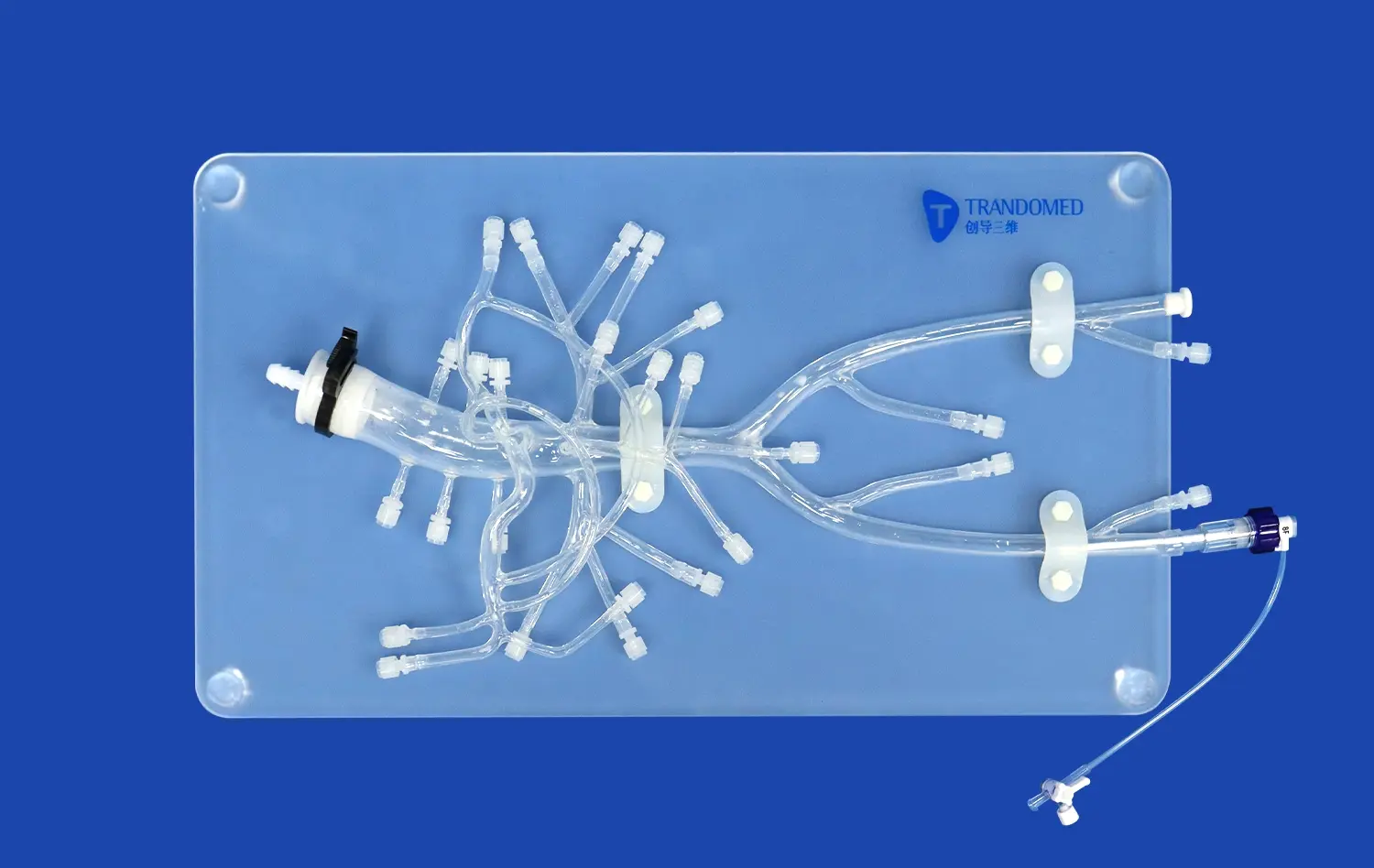
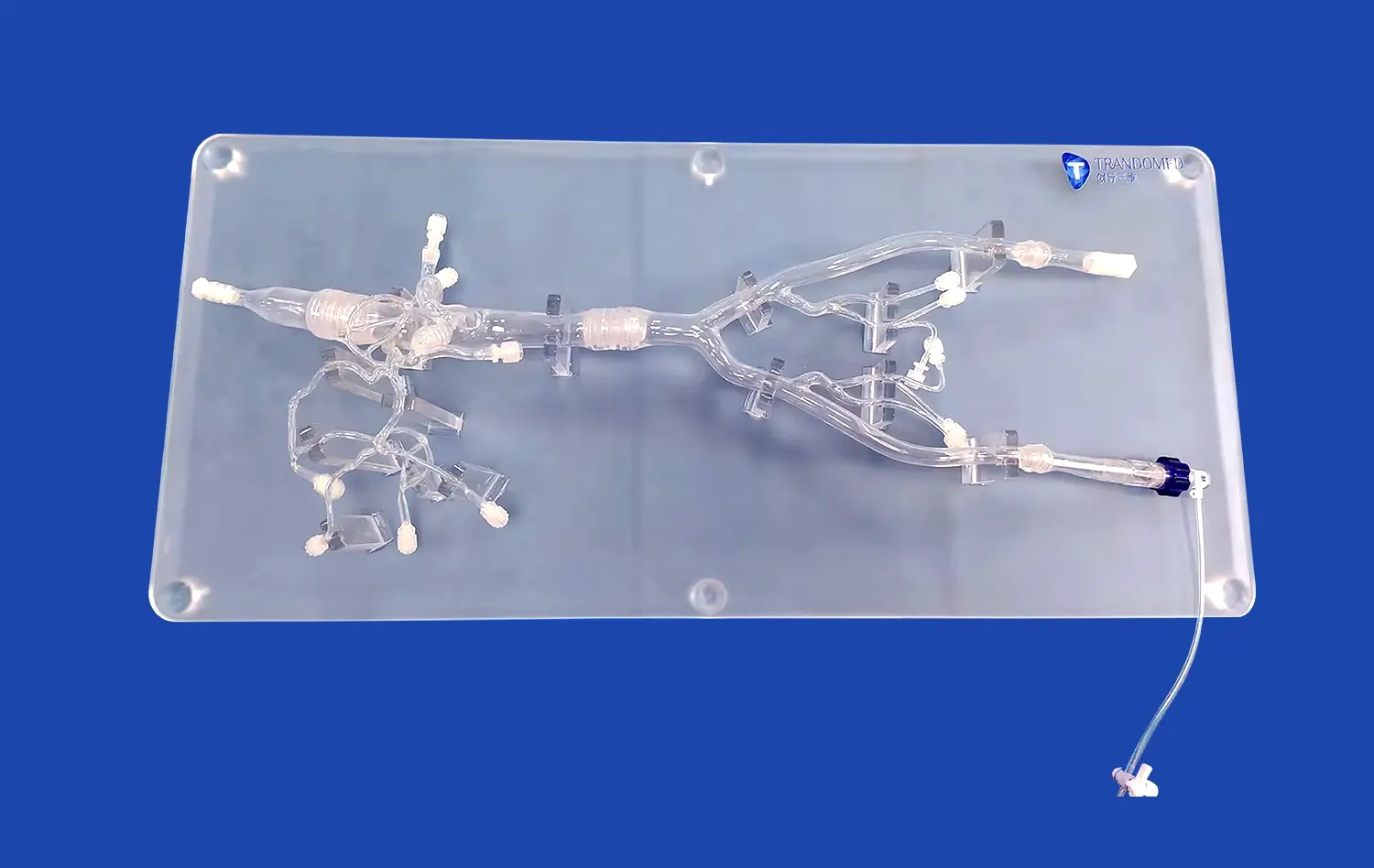
Trandomed has been making medical 3D printers better for over 20 years, and the Left Atrial Appendage Closure Simulator (Product XX013D) is the result of all of their work. This advanced training model carefully copies the heart's structure from the femoral vein entry point to the iliac vein, inferior vena cava, right atrium, interatrial septum, left atrium, left atrial appendage, and pulmonary veins. The dimensions of every anatomical structure are accurate thanks to large CT and MRI files. This makes sure that trainees learn about space and gain technical skills that can be used right away in clinical practice.
This model is unique because it can be used in a lot of different ways thanks to its modular component design. The model includes all four LAA shapes—chicken wing, cactus, windsock, and cauliflower—as separate parts that can be swapped out for each other. This way, training can cover all the different body types that come up in real life. Three replaceable atrial septal defects of different sizes also allow realistic transseptal puncture training, which is an important technical part of LAA closure techniques. With this modular method, a single simulator can be turned into a full training platform that can support a wide range of skill levels and educational goals.
Here are the core advantages that make this cardiovascular training model invaluable for institutional programs:
- Anatomical Precision Through Advanced Imaging: Trandomed constructs every model using reverse 3D reconstruction technology applied to authentic human CT and MRI data. This methodology captures anatomical details with accuracy that traditional manufacturing approaches cannot achieve, providing trainees with realistic spatial relationships and structural proportions that prepare them for actual patient anatomy.
- Material Science Optimized for Realistic Haptics: The XX013D utilizes Silicone Shore 40A throughout its construction, a carefully selected material that replicates human tissue compliance and resistance characteristics. This material choice ensures that catheter navigation, wire manipulation, and device deployment generate tactile feedback similar to actual procedures, developing the refined touch sensitivity that distinguishes expert operators.
- Comprehensive Procedural Scope: Beyond LAA closure training, this versatile platform supports transseptal puncture technique development, pulmonary vein ablation access practice, and general structural heart intervention skills. Training programs gain a multi-functional tool that addresses numerous curricular objectives within a single investment, maximizing educational value and equipment utilization.
- Customization Without Design Fees: Trandomed accepts patient-specific customization requests based on provided imaging data in CT, CAD, STL, STP, and STEP formats without charging additional design costs. This flexibility enables institutions to create rehearsal models for particularly complex cases or to replicate specific anatomical variants relevant to their patient populations.
These advantages collectively address the most challenging aspects of interventional cardiology training, creating a platform where repetitive practice builds both technical proficiency and clinical judgment. The combination of anatomical accuracy, material realism, procedural versatility, and customization capabilities positions the XX013D as a comprehensive solution for organizations committed to excellence in cardiovascular education.
Applications Across Medical Education and Clinical Environments
The XX013D simulator serves multiple critical functions throughout the medical education continuum and clinical practice settings. Medical schools utilize these models to introduce cardiovascular anatomy and basic catheter skills before students enter clinical rotations, building foundational competencies that accelerate subsequent learning. Residency and fellowship programs integrate the simulator into structured curricula that progressively develop technical proficiency from basic wire manipulation through complete procedural execution. Experienced practitioners use patient-specific customized versions for pre-operative rehearsal, particularly when confronting unusual anatomical configurations or planning complex revision procedures.
Device manufacturers have discovered significant value in these anatomically accurate models for product development, testing, and commercial applications. Engineering teams evaluate prototype devices under realistic anatomical conditions before committing to expensive production tooling. Clinical specialists conduct physician training workshops where the simulator's standardized anatomy ensures consistent educational experiences across multiple training sessions. Sales teams demonstrate device features and implantation techniques to potential customers in compelling, hands-on formats that static presentations cannot match. Research institutions employ these models for biomechanical studies, device comparison investigations, and technique optimization projects that advance the field.
Procurement Considerations and Customization Capabilities
Trandomed streamlines the procurement process through transparent specifications, efficient production timelines, and flexible customization options. The standard XX013D model ships within seven to ten days following order confirmation, utilizing reliable international carriers including FedEx, DHL, EMS, UPS, and TNT to ensure timely delivery to institutions worldwide. Payment processing through T/T arrangements provides straightforward financial transactions that align with institutional procurement protocols.
Customization capabilities extend beyond the standard modular configuration to include patient-specific anatomical replication, modified ASD positioning and dimensions, and specialized structural variations that address unique training requirements. Organizations simply provide imaging data in standard medical or engineering formats, and Trandomed's experienced design team translates this information into precision 3D-printed models. This personalization service, offered without additional design fees, transforms the XX013D from an excellent standard training tool into a perfectly tailored solution for specific institutional objectives, research protocols, or clinical rehearsal needs.
Purchasing Guide: Making Informed Simulator Acquisition Decisions
Technical Evaluation Framework for Procurement Teams
Procurement managers evaluating cardiovascular simulation solutions should establish a systematic assessment framework that examines multiple performance dimensions. Anatomical accuracy verification requires comparison against reference imaging datasets and validation by clinical subject matter experts who can assess dimensional precision and structural relationships. Material property evaluation should include hands-on testing by intended users who can judge tactile realism based on their clinical experience. Durability assessment examines expected component lifespan under typical training usage patterns, replacement part availability, and long-term cost of ownership beyond initial acquisition expenses.
Compatibility considerations ensure seamless integration within existing training environments. Left atrial appendage closure simulators should accommodate standard clinical imaging equipment without requiring specialized adaptations that limit flexibility or increase costs. Physical dimensions must fit available training space configurations while allowing adequate room for multiple participants during teaching sessions. Storage requirements affect space utilization when simulators are not actively deployed. These practical considerations significantly impact the actual utility that institutions realize from their simulation investments.
Vendor Assessment and Partnership Considerations
Selecting a simulation technology vendor involves evaluating not only product quality but also the broader partnership value that suppliers provide. Established manufacturers with extensive track records in medical simulation demonstrate technical expertise and operational stability that reduce procurement risk. Manufacturing quality certifications and regulatory compliance documentation verify that products meet healthcare industry standards for safety and performance. Customer references from comparable institutions provide insights into actual user experiences, implementation challenges, and long-term satisfaction that marketing materials cannot convey.
Post-purchase support capabilities strongly influence total ownership experience and value realization. Comprehensive technical documentation, training resources, and user guides facilitate rapid implementation and optimal utilization. Responsive customer service teams that understand clinical applications provide valuable troubleshooting assistance and consultation support. Clear warranty terms protect institutional investments against manufacturing defects and premature component failures. Software update policies for digitally enhanced simulators ensure that technology remains current as capabilities evolve. These service dimensions often differentiate vendors more significantly than initial product specifications alone.
Building a Business Case for Simulation Investment
Securing institutional funding for advanced simulation technology requires compelling business cases that demonstrate both educational value and financial return. Effective proposals quantify training volume capacity, calculating per-procedure costs that compare favorably against alternative training methods. Quality improvement metrics link enhanced operator proficiency to measurable outcomes including reduced complication rates, shorter procedure times, and improved first-attempt success rates. These clinical benefits translate to financial impact through decreased length of stay, lower complication treatment costs, and enhanced procedural throughput that increases revenue capacity.
Strategic positioning emphasizes competitive differentiation and institutional reputation benefits. Leading medical schools attract top students and faculty by offering superior educational resources and innovative training methodologies. Hospitals competing for complex case referrals demonstrate commitment to procedural excellence through investments in advanced training infrastructure. Device manufacturers gain competitive advantages by supporting product adoption through comprehensive physician education programs. These strategic considerations justify simulation investments beyond purely financial calculations, recognizing the broader organizational value that cutting-edge training capabilities provide.
Future Trends Shaping Cardiovascular Simulation Technology
Artificial Intelligence and Adaptive Learning Integration
The next generation of cardiovascular simulation platforms will incorporate artificial intelligence algorithms that personalize training experiences based on individual learner performance. These intelligent systems will analyze technical execution patterns, identify specific skill deficiencies, and automatically adjust scenario difficulty to maintain optimal challenge levels that promote rapid skill acquisition. Performance analytics dashboards will provide learners and educators with detailed insights into competency development, highlighting areas requiring additional practice and documenting progress toward proficiency benchmarks. This data-driven approach transforms simulation from a passive practice tool into an active educational partner that accelerates learning and ensures comprehensive skill development.
Augmented and Virtual Reality Enhancement
Augmented reality overlays and fully immersive virtual reality environments are expanding simulation capabilities beyond physical models. These technologies enable visualization of anatomical structures from any perspective, display real-time guidance information during procedures, and create standardized training scenarios that precisely replicate specific clinical situations. Hybrid approaches that combine physical left atrial appendage closure simulators with digital enhancement offer compelling advantages by preserving tactile realism while adding informational layers that enrich learning experiences. Remote proctoring capabilities enabled by these technologies allow expert instructors to observe trainee performance and provide guidance regardless of geographic separation, democratizing access to specialized expertise.
Patient-Specific Planning and Predictive Analytics
Advanced simulation technology increasingly supports pre-procedural planning through patient-specific modeling combined with predictive analytics. Sophisticated algorithms analyze individual anatomical configurations to recommend optimal device selections, predict deployment challenges, and suggest alternative approaches when standard techniques may prove difficult. These decision support tools augment physician judgment rather than replacing clinical expertise, providing evidence-based guidance that enhances procedural outcomes. Organizations investing in simulation infrastructure should prioritize platforms offering upgrade pathways that accommodate these emerging capabilities, protecting their investments against technological obsolescence.
Conclusion
Advanced cardiovascular simulation for left atrial appendage closure has transformed from an optional enhancement into an essential component of comprehensive training programs. The combination of anatomical precision, procedural versatility, and risk-free repetitive practice creates learning environments that traditional methods cannot match. Organizations seeking simulation solutions should evaluate technical specifications, assess vendor capabilities, and align investments with their specific educational objectives and learner populations. The Trandomed XX013D exemplifies how thoughtful design, advanced manufacturing, and clinical insight combine to deliver training tools that measurably improve operator competency and patient outcomes. As cardiovascular procedures continue increasing in complexity and patient expectations for safety intensify, simulation-based preparation will only grow in importance for institutions committed to clinical excellence.
FAQ
What is a left atrial appendage closure procedure?
Left atrial appendage closure is a minimally invasive or surgical procedure that seals off the LAA, a small sac extending from the left atrium's muscle wall. This intervention reduces stroke risk in patients with atrial fibrillation by preventing blood clot formation within the appendage. The procedure offers an alternative to lifelong anticoagulation therapy, particularly benefiting patients who cannot tolerate blood thinners due to bleeding risks or other contraindications.
What are the four types of left atrial appendage morphologies?
Large imaging studies have classified four main LAA morphologies based on structural characteristics. The chicken wing type, found in approximately 48% of patients, features a distinctive bend in the appendage. The cactus morphology appears in 30% of cases with multiple lobes extending in various directions. The windsock configuration occurs in 19% of patients as a single dominant lobe. The cauliflower type, present in only 3% of cases, displays complex internal trabeculations without a clear dominant structure.
How do simulation models improve procedural outcomes?
Cardiovascular simulation models enable practitioners to develop technical skills and procedural judgment through repetitive practice without patient risk. This hands-on experience builds muscle memory, refines catheter manipulation techniques, and enhances spatial awareness within cardiac anatomy. Patient-specific rehearsal using customized models allows clinicians to anticipate challenges and develop strategies before actual procedures, directly translating to reduced operative times and fewer complications.
Partner with a Trusted Left Atrial Appendage Closure Simulator Manufacturer
Trandomed stands as a pioneering left atrial appendage closure simulator supplier with over two decades of specialized experience in medical 3D printing technology. Our XX013D model delivers the anatomical accuracy, material realism, and procedural versatility that leading medical education institutions, hospital training departments, and device manufacturers demand. We combine proprietary 3D printing techniques, extensive human imaging databases, and rigorous quality assurance to manufacture simulators that elevate cardiovascular training programs. Our commitment extends beyond product delivery through comprehensive customization services, rapid production timelines, and dedicated technical support that ensures your complete satisfaction. Contact jackson.chen@trandomed.com to discuss your specific training requirements, request a detailed product demonstration, or explore how our customization capabilities can address your unique educational objectives and advance your institutional mission.
References
Di Biase L, Santangeli P, Anselmino M, et al. Does the left atrial appendage morphology correlate with the risk of stroke in patients with atrial fibrillation? Results from a multicenter study. Journal of the American College of Cardiology. 2012;60(6):531-538.
Holmes DR, Reddy VY, Turi ZG, et al. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial. The Lancet. 2009;374(9689):534-542.
Alkhouli M, Friedman PA. Ample room for improvement: Enhancing the quality and safety of left atrial appendage occlusion. JACC: Cardiovascular Interventions. 2018;11(14):1385-1387.
Barsness GW, Dahle TG, DeMartini TJ, et al. Use of simulation-based education to improve outcomes of central venous catheterization: A systematic review and meta-analysis. Academic Medicine. 2016;91(9):1288-1299.
Grantcharov TP, Kristiansen VB, Bendix J, et al. Randomized clinical trial of virtual reality simulation for laparoscopic skills training. British Journal of Surgery. 2004;91(2):146-150.
Meier B, Blankenship JC, Frey N, et al. Standardization of training in percutaneous left atrial appendage closure using simulation. EuroIntervention. 2016;12(7):e948-e954.

_1732863962417.webp)