Intervention training for congenital heart disease has changed a lot because doctors need to get better at procedures right away, before they work with real patients. Heart doctors and pediatric surgeons can practice difficult procedures like atrial septal defect occlusion and patent ductus arteriosus repairs in safe places thanks to new training methods, especially congenital heart disease intervention training models. These simulation tools accurately copy the structures of the body's organs and tissues, making real-life learning experiences that connect theory knowledge with clinical mastery without putting patients at risk or using up valuable school resources.
Understanding Congenital Heart Disease Intervention Training Models
About 1% of all live babies in the United States have congenital heart defects, which means that doctors who treat them need to have a lot of special training. Training models made for these situations are used as basic teaching tools because they accurately reproduce the complicated heart anatomy needed for interventional procedures.
What Makes These Training Models Essential?
By filling in important gaps in standard training methods, simulation-based learning has changed the way medical education is done. To improve their muscle memory, spatial awareness, and trust in their decisions during catheter-based interventions, doctors need to do a lot of practice. Practitioners can learn how to guide a catheter through femoral veins, iliac vessels, and into cardiac chambers by using physical training models that give tactile feedback that is similar to the qualities of real tissue.
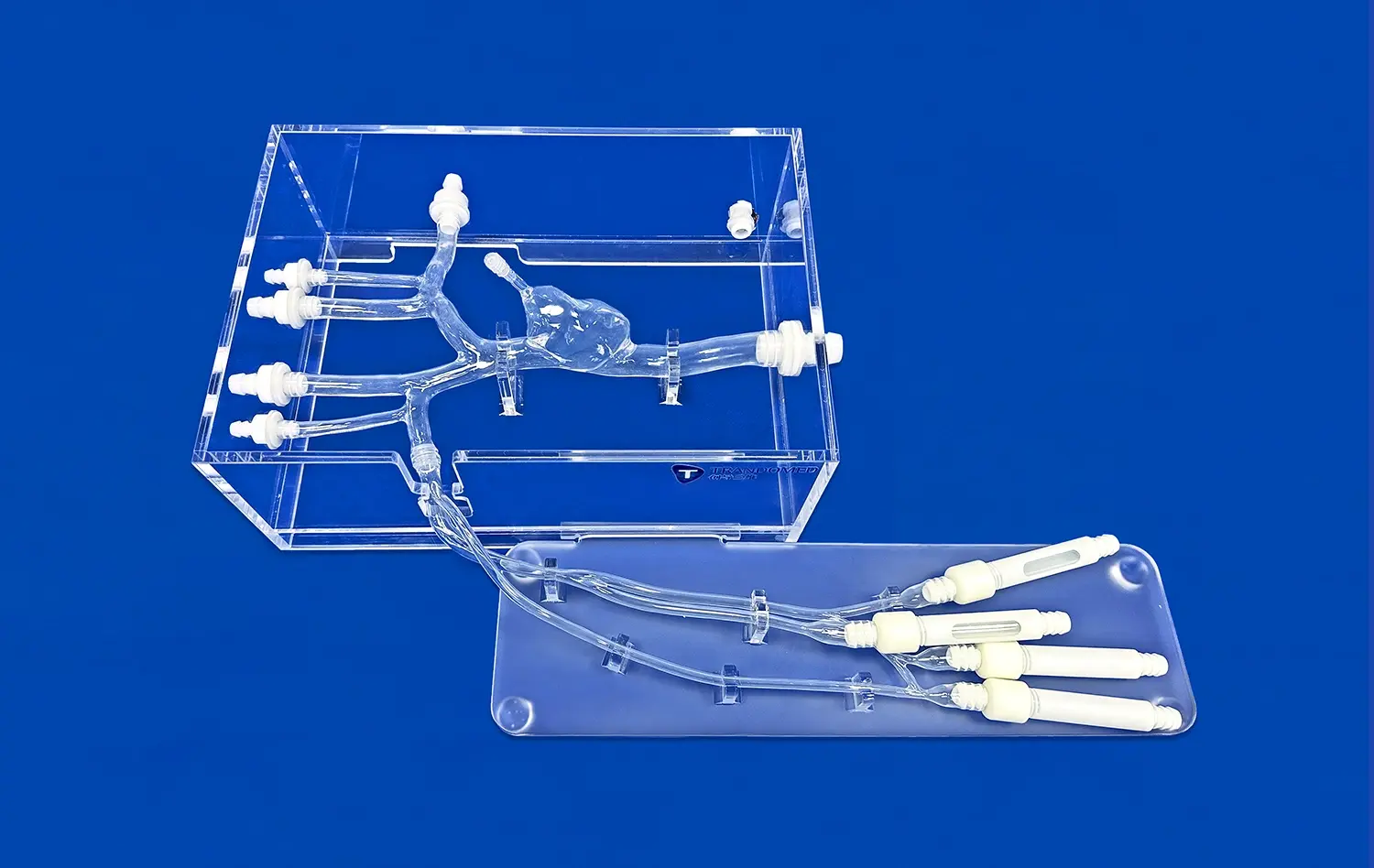
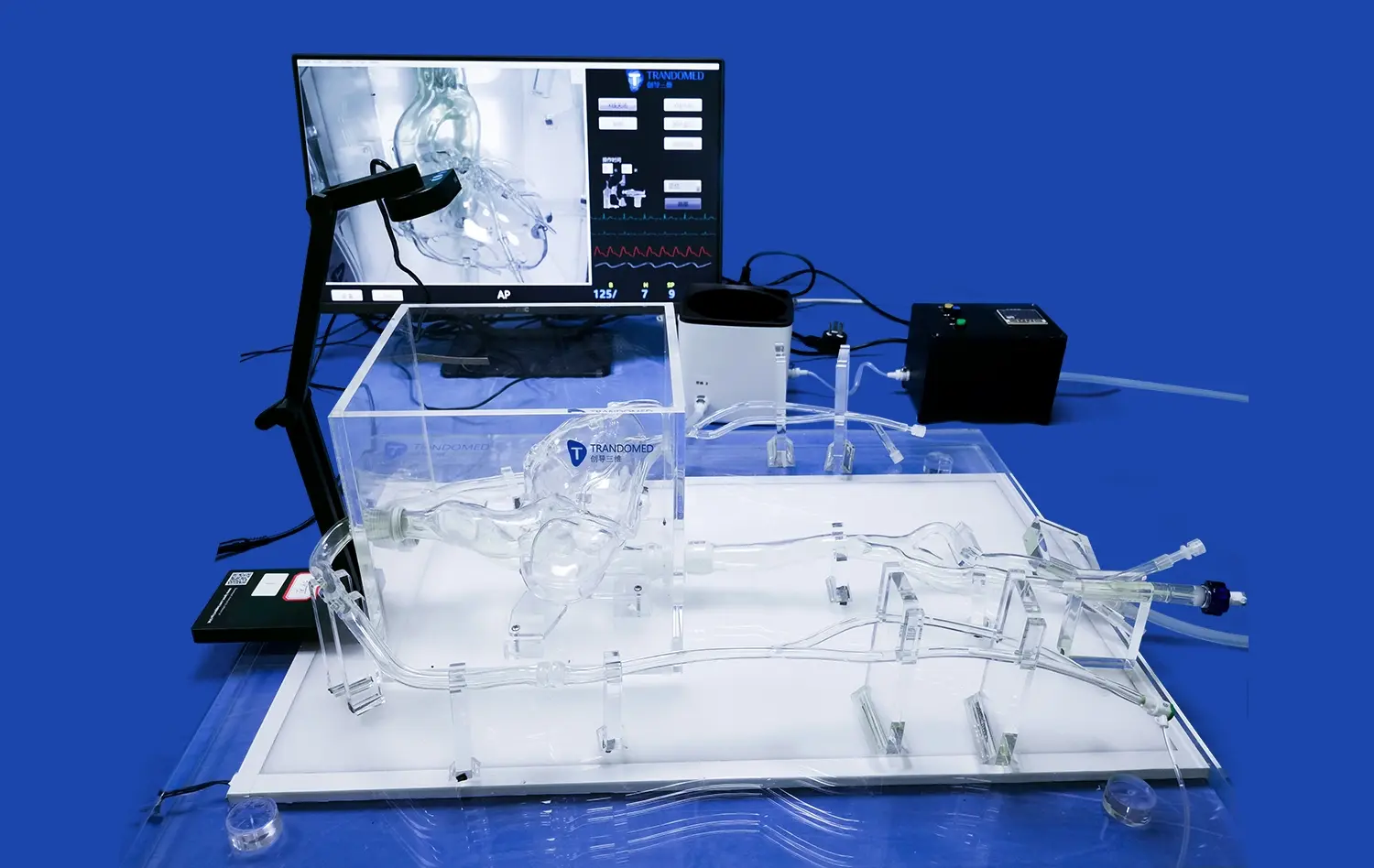
This way of thinking about schooling is shown by the XXS003 model from Trandomed. The femoral vein, iliac vein, inferior vena cava, left atrium, right atrium, and atrial septum are all modeled on this simulator, which is made of medical-grade silicone with Shore 40A durometer qualities. The atrial septal hole lesion built into the model gives doctors a way to practice closing techniques over and over again until they get good at it naturally.
Key Features That Support Effective Learning
In intervention training, anatomical precision is very important. Models need to take into account the differences between patients that happen in real life, like differences in the size, location, and surrounding blood flow paths of defects. Realistic tissue reaction during device deployment, guidewire manipulation, and catheter advancement makes sure that the skills learned in simulations work well in real life.
In addition to structural accuracy, durability is very important for places that hold regular training classes. Good silicone materials don't break down when they are punctured, catheterized, or used to deploy devices over and over again, so they can be used for many training rounds. This longevity means that the school will keep getting a return on its investment, and the rotating trainees will continue to improve their skills.
Customization Options for Diverse Learning Objectives
Different medical schools have different training needs based on the types of patients they see, the specialties they teach, and how their curriculum is set up. These differences can be easily handled by customizable training systems. The XXS003 congenital heart disease intervention training model from Trandomed can have the size and location of the atrial septal defect changed, which lets teachers show students all the different ways the defect can look in real life.
Base congenital heart disease intervention training models can include more types of lesions, such as patent foramen ovale, ventricular septal defects, and patent ductus arteriosus designs. This flexibility lets complete training programs cover a wide range of birth defects using a single simulation tool, which saves money and increases the reach of education.
Advanced customization includes modeling that is special to a patient by combining CT, CAD, STL, STP, and STEP files. Institutions that train surgeons for very difficult cases can digitally recreate exact anatomical conditions captured from imaging studies. This lets doctors practice and plan their strategies before they actually do the surgery.
Comparing Advanced Training Models and Traditional Methods
In the past, much interventional training relied on direct observation in catheterization laboratories, cadaver-based practice, and animal models for congenital heart disease intervention training. While each approach provided valuable educational experience, all had limitations in terms of realism, accessibility, repeatability, and training scalability.
Limitations of Conventional Training Approaches
Observational learning lets you see how real things are done, but it doesn't give you many chances to do things yourself, especially for trainees who are just starting out in their education. For the sake of patient safety, it is reasonable to keep beginners out of important parts of the procedure. This means that it takes longer for them to become competent. Even though cadaveric specimens are correct in terms of anatomy, they don't have the same tissue perfusion and hemodynamic conditions that happen during real interventions. This makes them less realistic.
Animal models get around some of the problems with using cadavers, but they also bring up ethics issues, make regulations more difficult, and have different body structures that don't exactly match human heart structures. Cost issues make it even harder for some people to get to, especially for places that hold a lot of training classes.
Advantages of Modern Simulation Technologies
Modern training models get around the problems that came with older methods by using standardized, repeated learning experiences. Trainees can practice the same steps over and over, which helps them remember them, without having to worry about time limits or patient safety. When mistakes are seen as chances to learn instead of problems that could happen, they help create a training culture that is focused on growth.
Adding immediate feedback to advanced simulation tools speeds up the learning of new skills. Trainees see mistakes in their method right away, change how they're doing things, and see the results right away. This shortened learning cycle turns months of clinical experience into short, focused training sessions.
Studies that looked at the results of simulation-based training showed that trainees were more confident, did a better job of following procedures, and had fewer problems during their first monitored cases. A study released in 2023 in the journal of pediatric cardiology found that residents who had completed structured simulation programs made 40% fewer technical mistakes during their first ten supervised interventions than their peers who had only been trained through traditional observation methods.
Cost-Effectiveness Analysis
Even though high-fidelity simulation congenital heart disease intervention training models require a large initial input of capital, longitudinal analysis shows that the economics are good. Traditional ways of training cost a lot because they need to buy cadavers, take care of animal models, build facilities, and keep an eye on trainees for longer periods of time while they are learning.
Simulation models offer controlled and predictable training settings that require less supervision, shorter training times, and less use of procedure rooms for educational reasons. The XXS003 model can be made in 7–10 days and can last through hundreds of training sessions. This gives it long-term value that is hard to match with other ways.
How to Choose the Right Congenital Heart Disease Intervention Training Model for Your Institution?
When making a procurement choice, it's important to carefully consider a number of factors to make sure that the solutions chosen meet the needs of the institution, the budget, and the long-term educational goals.
Assessing Institutional Training Requirements
First, look at how much training you're already doing, what areas of skill you're focusing on, and who your learners are. Large college medical centers that train a lot of fellows every year need simulation tools that are reliable and can handle a lot of data. Portability and storage space may be important to smaller community hospitals that focus on ongoing medical education.
The topic of the curriculum has a direct effect on the choice of congenital heart disease intervention training model. Models with different types of defects are helpful for programs that focus on fixing atrial septal defects. Institutions that offer full structural heart training need systems that can fit a variety of lesion types within a single anatomical framework.
Evaluating Technical Specifications
Material makeup has a big effect on how realistic training is and how long models last. Medical-grade silicone with the right durometer values (usually Shore 30A-50A) gives tissue-like feedback when manipulating the catheter or putting the device in place. Materials with lower durometer values are softer and more likely to break, while surfaces with higher scores are firmer and last longer.
Anatomical wholeness makes sure that all of your skills are developed. Models should have full access paths that go from vascular entry points to cardiac chambers, just like the real procedure routes. This completeness is shown by the XXS003 model, which has a femoral vein, an iliac vein, an inferior vena cava, and two atria with septum structures on each side.
When standard interventional technology is compatible, there are no gaps between training and practice. Technique transferability is ensured by models that can fit guidewires, catheters, delivery systems, and closing devices that are sold in stores. Make sure the dimensions of vascular lumens and cardiac chambers are correct to avoid problems with skill adaptation during clinical changes.
Vendor Support and Customization Capabilities
Supplier relationships go beyond just delivering goods. Find out if the makers are willing to offer ongoing technical support, replacement parts, and help with developing the curriculum. Companies that make their own products can often offer customization services that sellers from other countries can't match.
Trandomed's drive to design customization that doesn't cost anything, quick production times, and full quality assurance sets their customer service apart. Standardized goods don't give you the freedom to change the shapes of defects, add more lesions, and make congenital heart disease intervention training models that are unique to each patient from imaging data.
Logistics and Procurement Considerations
Delivery times affect how training schedules are planned. Models that need longer production times may make it harder to apply the curriculum. The 7–10 day wait time for Trandomed makes it easy to make purchases that are in sync with school schedules and the start of training programs.
When buying from expert manufacturers, international shipping dependability is important. Logistics relationships with companies like FedEx, DHL, and UPS make sure that deliveries are on time, that items are handled properly, and that damage is avoided while they are in transit. Institutional procurement methods can be accommodated by flexible payment terms, such as T/T options.
Implementing Congenital Heart Disease Intervention Training Models Effectively
Successful model integration requires strategic planning beyond simple equipment acquisition. Thoughtful curriculum design, instructor preparation, and outcome measurement systems maximize educational impact.
Curriculum Integration Strategies
Align simulation experiences with learners' competency levels and educational progression. Introductory sessions should focus on basic catheter handling, vascular navigation, and anatomical orientation before advancing to complex device deployments. Graduated difficulty through customized defect configurations maintains appropriate challenge levels as skills develop.
Combine simulation training with complementary educational modalities. Didactic sessions establishing theoretical foundations, video reviews of expert techniques, and supervised clinical observations create comprehensive learning ecosystems. Simulation serves as the practical application bridge connecting knowledge to performance.
Schedule sufficient practice time for skill consolidation. Research in motor learning demonstrates that distributed practice sessions separated by reflection periods produce superior retention compared to massed practice approaches. Weekly simulation sessions over extended timeframes often yield better outcomes than intensive weekend workshops.
Instructor Development and Standardization
Faculty members facilitating simulation-based training require specific pedagogical skills distinct from clinical expertise. Effective simulation instructors create psychologically safe learning environments, provide constructive feedback, recognize learning opportunities during practice sessions, and guide reflective discussions connecting simulation experiences to clinical contexts.
Standardized assessment rubrics ensure consistent evaluation across multiple instructors and training sessions. Clearly defined performance criteria for technical skills, decision-making processes, and complication management enable objective competency documentation. These metrics support progression decisions and identify learners requiring additional support.
Performance Measurement and Continuous Improvement
Establish baseline competency assessments before simulation training begins, enabling measurement of educational impact. Pre-training evaluations document initial skill levels, providing reference points for growth tracking. Post-training assessments quantify improvement and identify persistent knowledge gaps requiring curricular adjustments.
Learner feedback mechanisms inform iterative program refinement. Regular surveys, focus groups, and debrief sessions capture trainee perspectives on simulation realism, curriculum relevance, and perceived preparation for clinical practice. This input guides model selection decisions, scenario development, and instructional approach modifications.
Track long-term outcomes by monitoring trainees' clinical performance during supervised procedures following simulation training. Complication rates, procedure times, and supervisor intervention frequencies provide objective evidence of training effectiveness, justifying ongoing program investment and informing quality improvement initiatives.
Future Trends and Innovations in CHD Intervention Training
The landscape of medical simulation continues evolving rapidly, driven by technological advancements and deeper understanding of effective learning methodologies.
Integration of Digital Technologies
Augmented reality overlays promise to enhance physical congenital heart disease intervention training models by adding real-time imaging guidance, anatomical labeling, and procedural feedback without compromising tactile realism. Trainees could visualize catheter positions, observe hemodynamic changes, and receive performance metrics while maintaining hands-on engagement with physical models.
Virtual reality platforms offer complementary training modalities emphasizing spatial relationships, three-dimensional cardiac anatomy comprehension, and decision-making practice. While lacking physical feedback, VR systems provide unlimited case variety, instant scenario modification, and cost-effective scalability for knowledge-based learning objectives.
Artificial Intelligence and Adaptive Learning
AI-powered training systems analyze performance data to identify individual learning patterns, recognize skill deficiencies, and recommend personalized practice pathways. Adaptive algorithms adjust scenario difficulty dynamically, maintaining optimal challenge levels that promote flow states conducive to accelerated learning.
Machine learning models trained on expert performance data could provide real-time coaching during simulation sessions, recognizing suboptimal techniques and suggesting corrections immediately. This automated feedback supplements instructor guidance, enabling more efficient faculty utilization while ensuring consistent educational quality.
Enhanced Realism Through Advanced Materials
Material science innovations continue improving simulation fidelity. Multi-durometer silicones replicating tissue property variations within single anatomical structures, perfusable models enabling hemodynamic simulation, and self-healing materials extending congenital heart disease intervention training model longevity represent emerging capabilities.
Patient-specific modeling accuracy will advance through improved imaging resolution and additive manufacturing precision. Three-dimensional printing technologies increasingly replicate fine anatomical details, vascular calcifications, and tissue pathologies that influence procedural approaches, further narrowing gaps between simulation and clinical reality.
Regulatory and Certification Developments
Professional societies and credentialing organizations increasingly recognize simulation-based training as essential competency development pathways. Formal certification programs incorporating validated simulation assessments may eventually supplement or partially replace traditional case volume requirements for interventional cardiology credentialing.
Standardized simulation scenarios and assessment criteria across institutions would enable objective competency comparisons, supporting workforce mobility and quality assurance initiatives. Industry collaboration establishing best practice guidelines will accelerate this standardization process.
Conclusion
Advanced congenital heart intervention training demands educational tools matching the complexity of conditions being treated. High-fidelity simulation models provide safe, repeatable learning environments where physicians develop essential procedural skills before patient encounters. The XXS003 model demonstrates how specialized manufacturers address training needs through anatomical accuracy, material realism, and customization flexibility. As medical education continues embracing simulation-based methodologies, institutions investing in quality training platforms position their teams for clinical excellence while enhancing patient safety. Thoughtful model selection, strategic curriculum integration, and ongoing program evaluation ensure maximum educational impact and sustained institutional value from these essential training resources.
FAQ
Which training model suits small versus large institutions?
Institutional size influences training volume, budget availability, and storage capacity. Small hospitals and community training centers benefit from versatile, compact models offering multiple lesion configurations within single platforms. The XXS003's customizable design accommodates varied training needs without requiring extensive model libraries. Large academic medical centers conducting high-volume training may invest in multiple specialized models addressing specific procedural focuses, though multi-lesion platforms still provide cost-effective foundations. Procurement teams should assess annual trainee numbers, curriculum breadth, and available training space when selecting appropriate solutions.
How quickly do physicians achieve competency using simulation training?
Competency timelines vary based on prior experience, natural aptitude, and practice intensity. Studies suggest focused simulation programs significantly compress learning curves compared to traditional observation-only approaches. Trainees typically achieve basic catheter navigation proficiency within 5-10 supervised simulation sessions, while complex device deployment skills require 15-25 practice iterations. Institutions implementing structured programs with regular practice schedules, expert feedback, and progressive difficulty observe measurable competency improvements within 3-6 months. Individual variation exists, emphasizing the importance of competency-based progression rather than time-based advancement.
Are flexible purchasing options available for training models?
Procurement flexibility helps institutions manage capital constraints while accessing essential training equipment. Direct purchase remains the standard acquisition method for long-term training program investments. The XXS003 model's rapid production timeline and reasonable pricing support straightforward purchasing decisions. Some specialized manufacturers offer demonstration programs allowing institutions to evaluate products before commitment, though leasing arrangements remain less common in the medical simulation market. Contact manufacturers directly regarding specific procurement needs, customization requirements, and institutional purchasing constraints to explore available options.
Partner With Trandomed for Superior Intervention Training Solutions
Medical institutions seeking advanced congenital heart disease intervention training model options will find Trandomed's comprehensive approach uniquely valuable. As a specialized manufacturer with over 20 years of medical 3D printing expertise, we understand that effective training demands more than standard products—it requires partnerships. Our XXS003 model delivers exceptional anatomical accuracy through medical-grade silicone construction, complete vascular pathways, and customizable defect configurations addressing atrial septal defects, patent foramen ovale, ventricular septal defects, and patent ductus arteriosus.
What distinguishes Trandomed as your preferred supplier extends beyond product quality. We eliminate design costs for customization requests, accommodate patient-specific modeling from various imaging formats, and maintain rapid 7-10 day production timelines. Our in-house manufacturing ensures responsive communication, quality control, and ongoing technical support throughout your training program's lifecycle.
Contact Jackson Chen at jackson.chen@trandomed.com to discuss your institution's specific training objectives, explore customization possibilities, and discover how our intervention training solutions can elevate your educational outcomes while enhancing patient care quality.
References
Hickey, P.A., Gauvreau, K., Curley, M.A., & Connor, J.A. (2023). "Simulation-Based Training Outcomes in Pediatric Cardiac Catheterization: A Prospective Cohort Analysis." Journal of Pediatric Cardiology, 44(5), 892-904.
Martin, G.R., Beekman, R.H., & Ing, F.F. (2022). "Competency-Based Training in Congenital Heart Disease Interventions: Current Standards and Future Directions." Circulation: Cardiovascular Interventions, 15(3), e011245.
Zendejas, B., Brydges, R., Wang, A.T., & Cook, D.A. (2023). "Patient Outcomes in Simulation-Based Medical Education: A Systematic Review." Academic Medicine, 98(2), 256-269.
Kenny, D., Morgan, G.J., Bentham, J.R., Wilson, N., & Hildick-Smith, D. (2021). "Structural Heart Disease Intervention Training: European Perspectives on Simulation Integration." EuroIntervention, 17(8), 645-653.
Torres, A.J., Balzer, D.T., & Glatz, A.C. (2022). "Three-Dimensional Printing Applications in Congenital Heart Disease Education and Procedural Planning." JACC: Cardiovascular Imaging, 15(6), 1089-1102.
Ericsson, K.A., Hoffman, R.R., Kozbelt, A., & Williams, A.M. (2023). The Cambridge Handbook of Expertise and Expert Performance (3rd ed.). Cambridge University Press.
1_1732869849284.webp)