ASD Occlusion Training With Congenital Heart Disease Simulators
2026-05-22 09:00:04
A congenital heart disease intervention training model is necessary when training programs need solid ways to learn how to do procedures on people with atrial septal defects. The complicated anatomy and catheterization pathways needed for ASD occlusion are modeled by these simulation systems. This lets doctors practice over and over again without any risk. The technology fills in the gaps between what doctors know in theory and how confident they are in doing procedures in the real world. It also solves the problems with training that have long made it hard for young cardiologists to get hands-on experience.
Understanding Congenital Heart Disease Intervention Training Models
What Makes These Simulators Essential for Clinical Education?
The way we train interventional cardiologists and pediatric specialists has changed a lot thanks to modern modeling technology. Unlike cadaveric specimens or animal models, synthetic simulators offer consistent anatomy, repeatable scenarios, and zero ethical concerns. The feedback that trainees get when they move catheters through silicone vessels feels like real tissue resistance. This helps them build the muscle memory they need for delicate treatments.
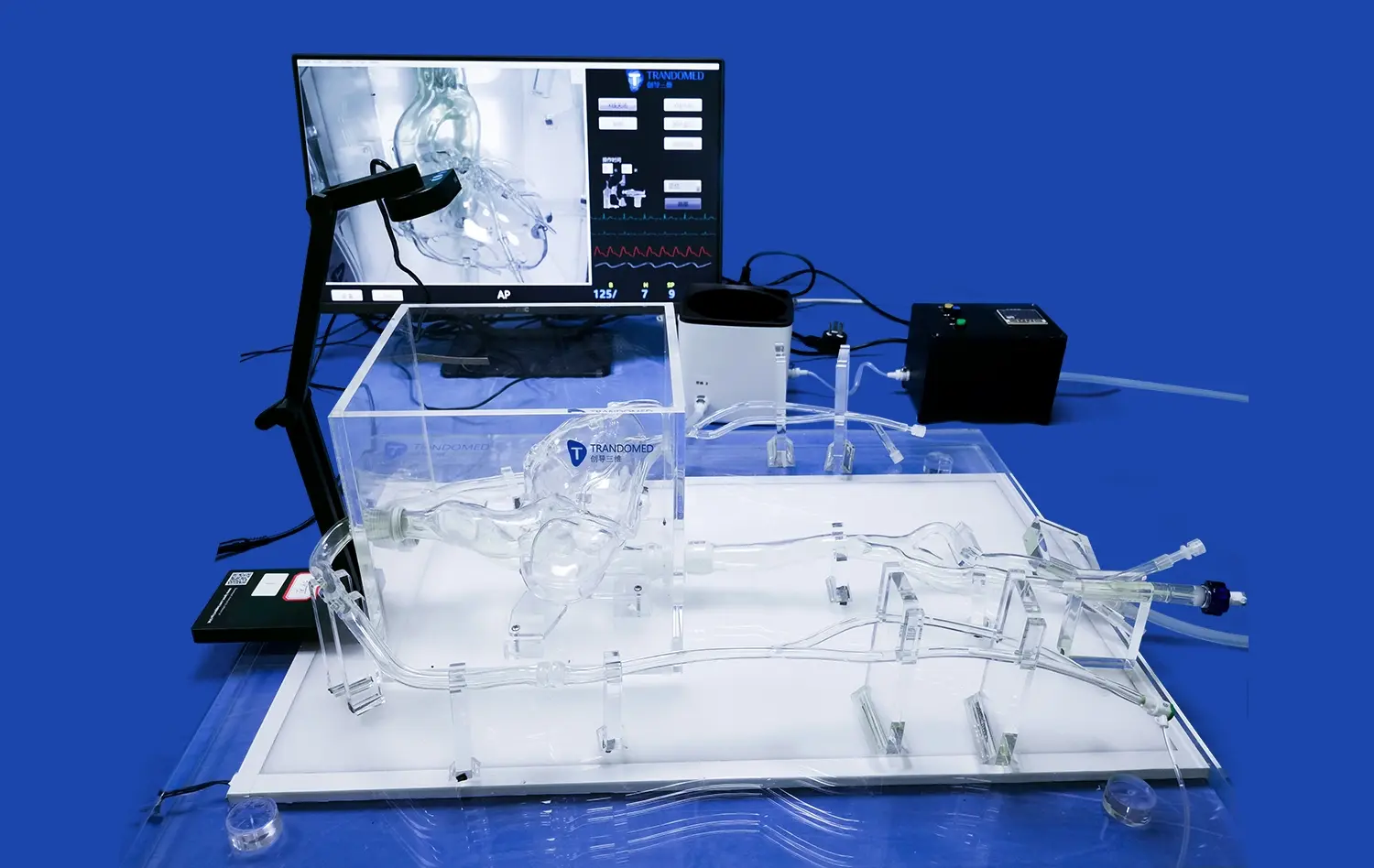
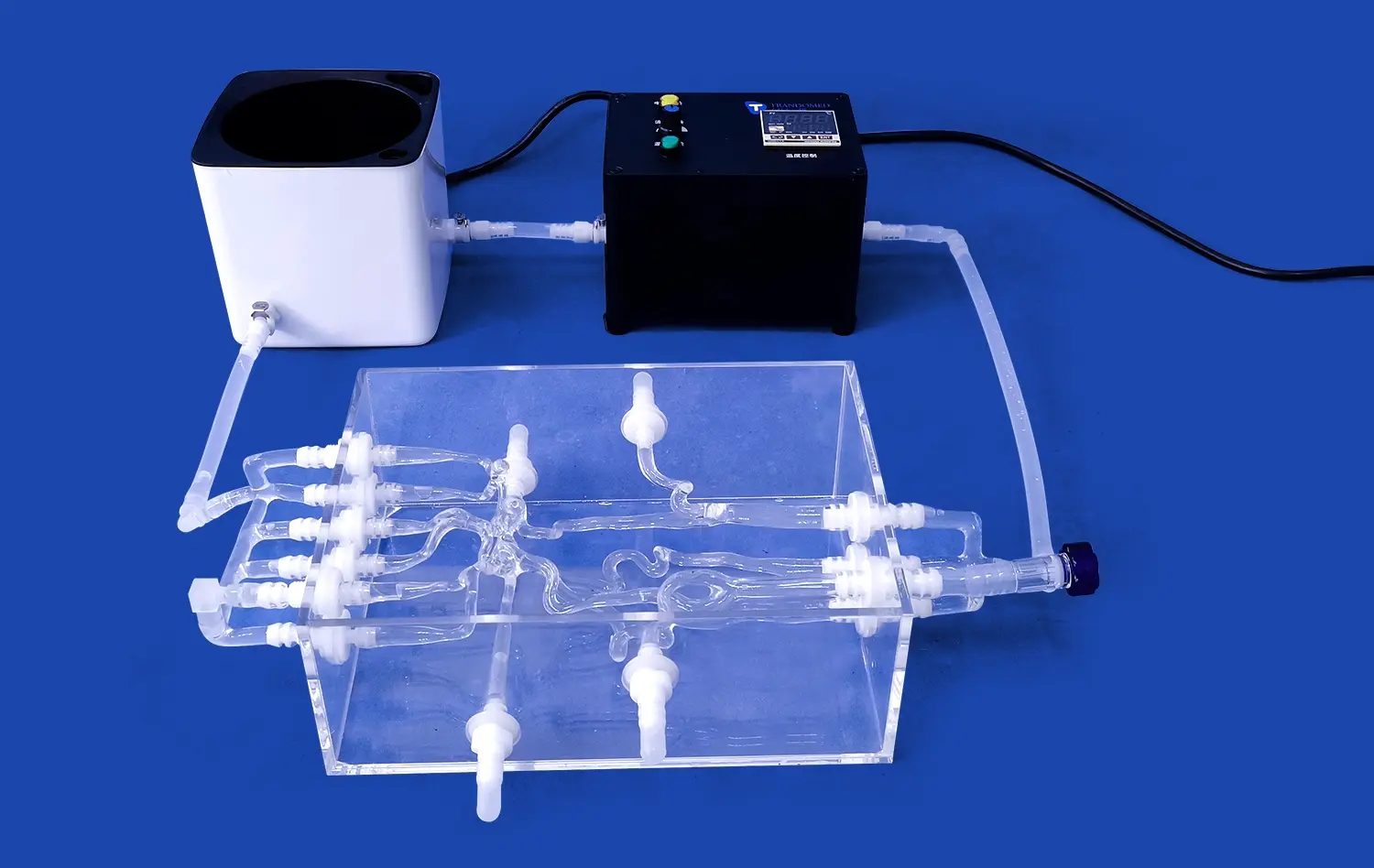
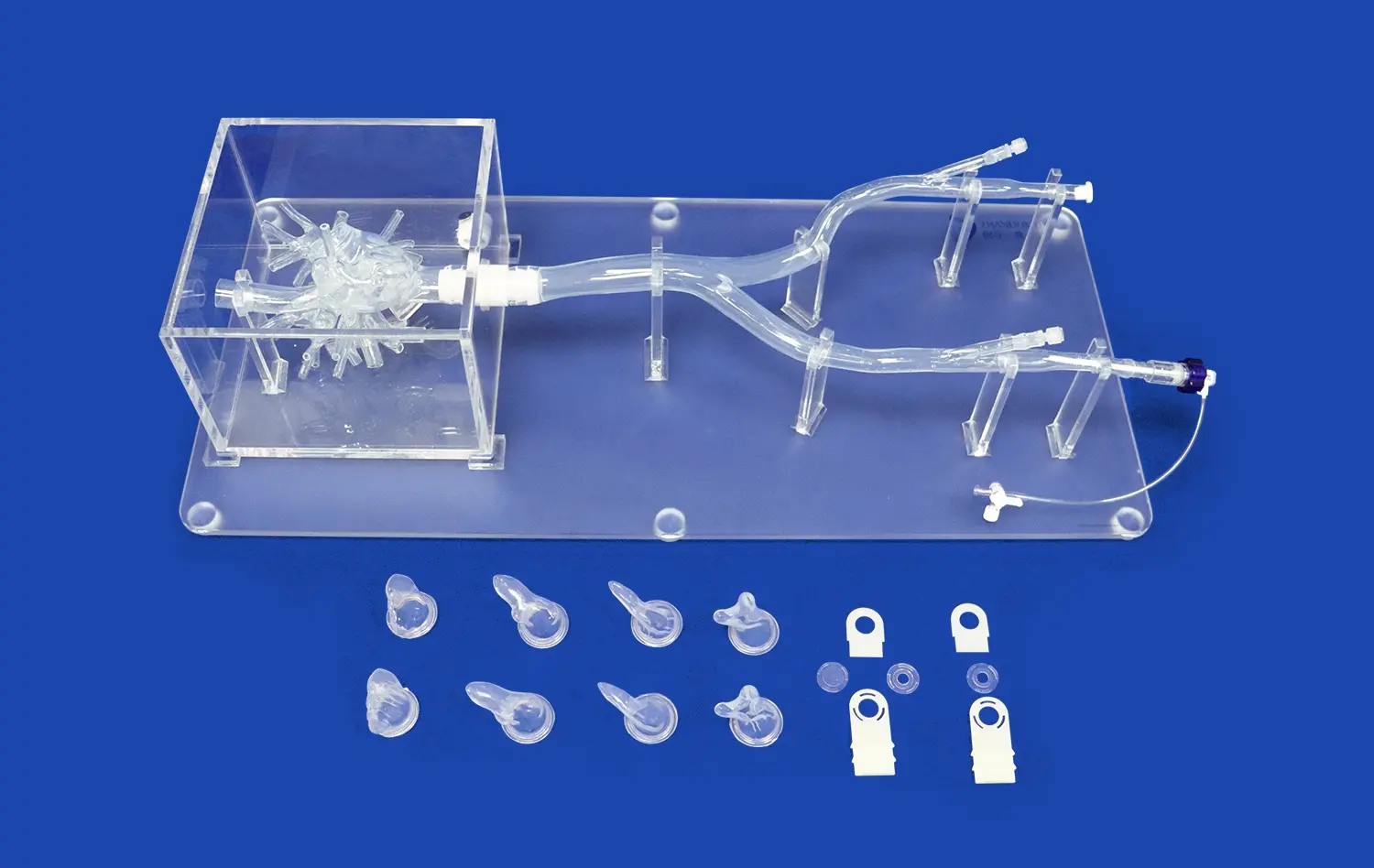
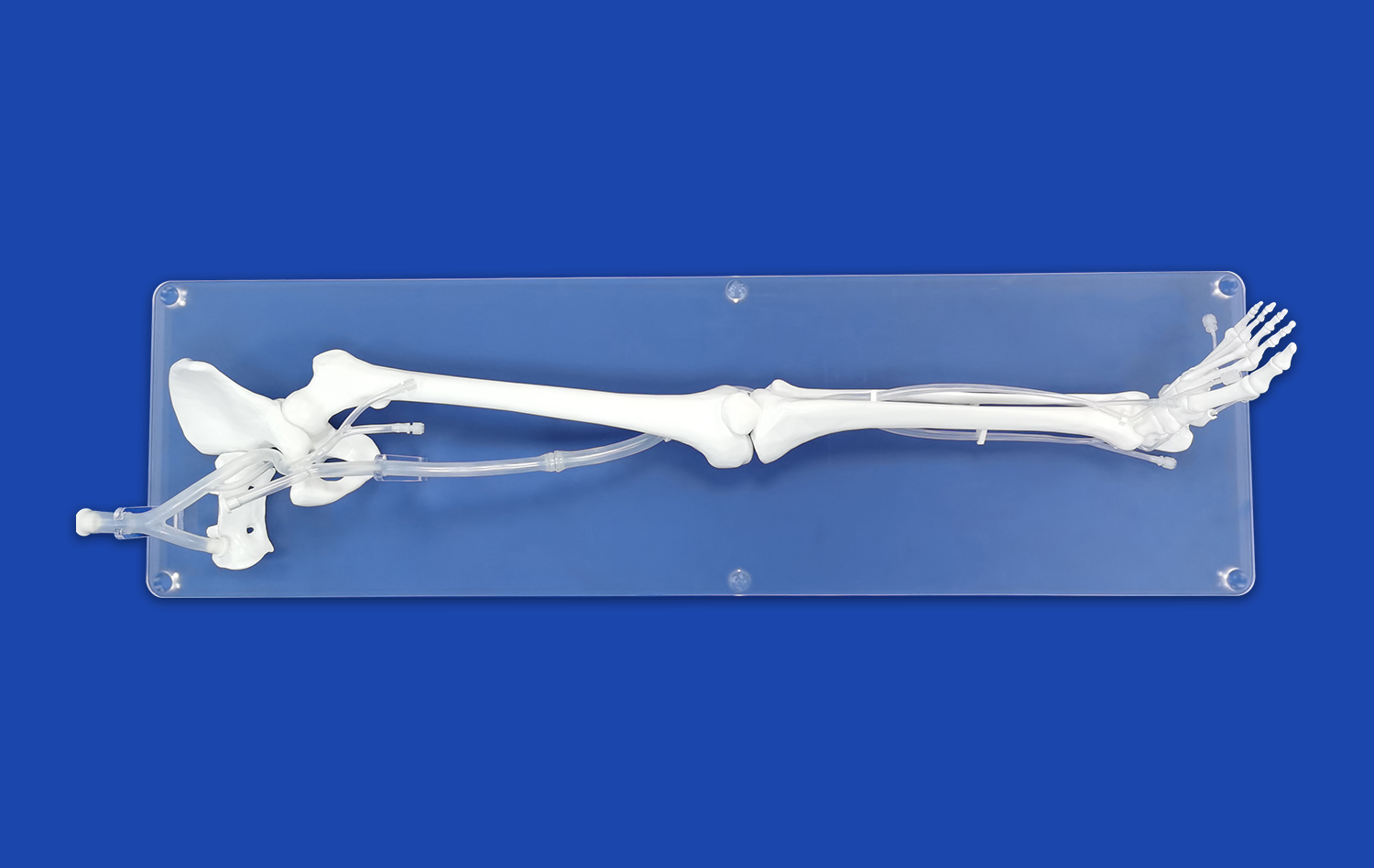
The femoral vein, the iliac vein, the inferior vena cava, and both cardiac chambers are all accurately modeled in our XXS003 model at Trandomed. The atrial septum has an ASD injury that can be moved and changed in size and position to meet specific training goals. At this level of physical accuracy, trainees will experience the same spatial relationships and technical difficulties that they will face when caring for real patients.
Core Components That Drive Training Effectiveness
The materials used in computer models have a big effect on how well training works. Shore 40A silicone, which is used in our XXS003, has mechanical qualities that are very close to those of human heart tissue. This choice of material makes sure that guidewires, delivery sheaths, and blocking devices work with the model the same way they would in real life.
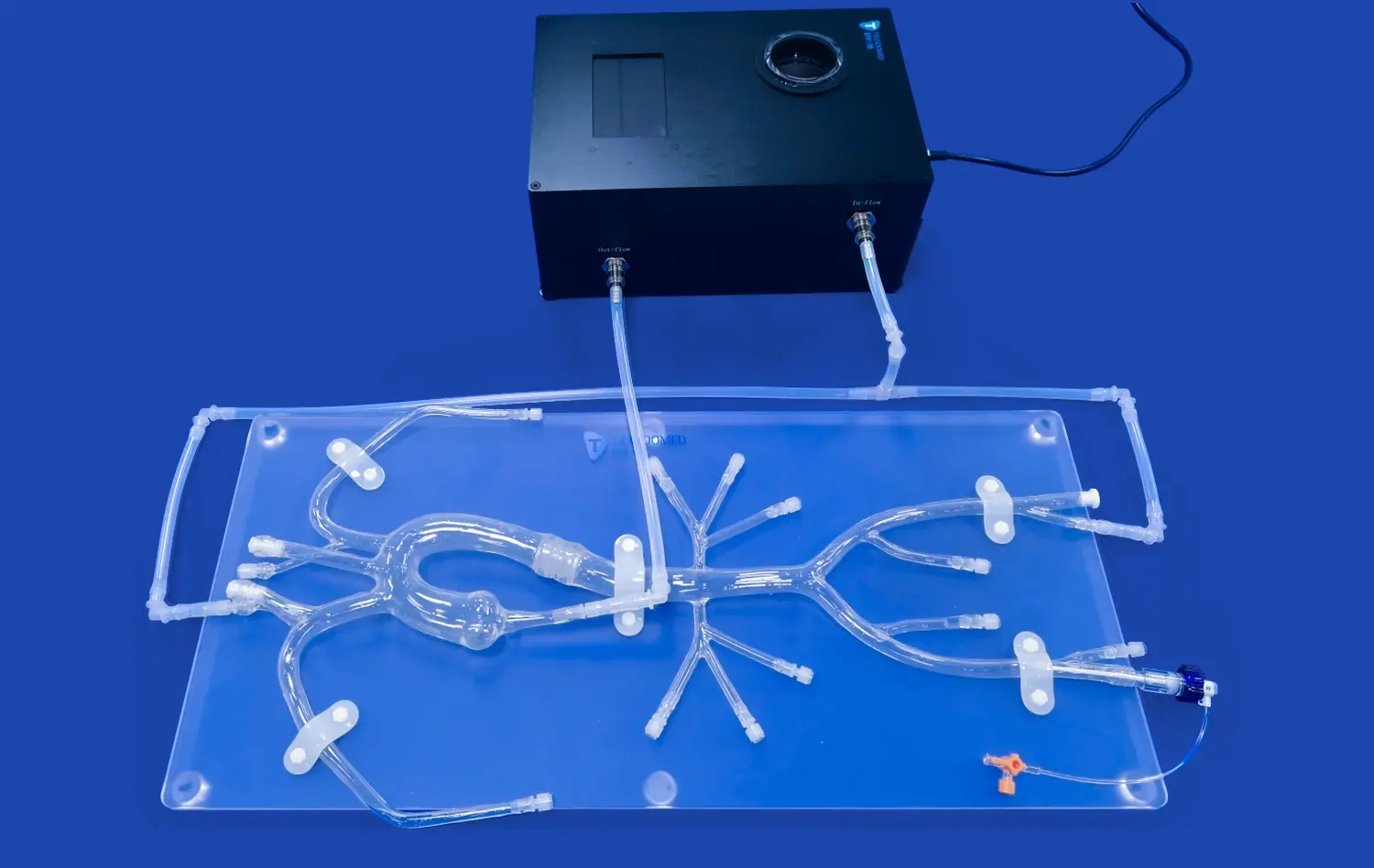
The blood flow line from the femoral access to the atrial septum is not easy to design. Trainees have to get through the iliac bifurcation, the IVC without cutting it, and the septal hole with the delivery system in the exact right place. Each anatomical landmark in the simulator is a learning opportunity that helps with spatial awareness in a way that is hard to do with just books or movies.
Comparing ASD Occlusion Training Models With Traditional Training Methods
Proctored procedures, in which younger operators help more experienced doctors during real cases, have been a big part of traditional training in interventional cardiology. Even though this apprenticeship approach is helpful, it limits the number of chances to learn and adds safety concerns for patients that make hands-on participation harder.
Limitations of Conventional Training Approaches
Observational learning doesn't give you much physical experience. Medical residents and fellows may watch dozens of treatments before they are allowed to touch or move medical devices themselves. This passive exposure slows down the growth of skills and can make training take longer than it needs to. Animal models have differences in anatomy that don't directly apply to human cardiac systems. This is especially true for children, whose sizes and proportions are very different from adults'.
You can't say enough about how unethical it is to learn on people. Even with expert direction, a trainee's learning curve can cause problems with the way things are done. Even though complications from lack of knowledge are rare, they can be very bad and lead to things like device embolization, cardiac perforation, or stroke.
Advantages of Simulation-Based Training Systems
This way of thinking is completely changed by simulator-based instruction. Trainees can practice methods over and over until they get it right, making mistakes that would be very bad for patients but are great for learning in a controlled setting. Being able to practice the whole process, from getting access to the blood vessels to putting the device in place and making sure it is in the right place, builds overall competence.
Studies in cardiac education magazines show that simulation training cuts down on mistakes by as much as 40% compared to the old ways of doing things. When operators go through organized simulator courses, their first supervised clinical cases have much shorter fluoroscopy times and fewer access problems. These numbers show how valuable the idea is for organizations that are thinking about investing in training.
Customers tell us that residents who learn on the XXS003 congenital heart disease intervention training model are more confident and accurate when they move on to proctored clinical procedures. The lifelike tissue feel and anatomical accuracy of the simulator make the change from training to real patient care less shocking.
Procurement Guide: How to Choose and Purchase ASD Occlusion Training Simulators
To choose the right simulation equipment, you need to carefully think about your long-term training goals, clinical needs, and finances. Medical schools, hospital training departments, and simulation centers have a lot of choices when it comes to purchasing things. These options range in price and capability.
Critical Selection Criteria for Institutional Buyers
Anatomical precision is the most important thing to think about. The simulator has to accurately show not only the target defect but also the whole catheterization route. Vascular dimensions, chamber shape, and tissue compliance are all things that affect how useful training is. When models of anatomy are too simple, they might teach skills that don't work well in real life.
Being able to customize a simulator makes it more useful for a wider range of training levels and procedure changes. Because defects can be changed in size, location, and complexity, a single model can be used for more than one teaching purpose. As part of our customization services, we can change the sizes and locations of ASDs, add other lesions such as patent foramen ovale, ventricular septal defects, or patent ductus arteriosus, and even make patient-specific models from CT or MRI data sent in standard formats like DICOM, STL, and STEP files.
When you figure out the total cost of ownership, durability is a big deal. A simulator that can be used hundreds of times without breaking down is a better deal than models that need to be replaced all the time. The silicone in our products keeps its mechanical properties even after a lot of use. Institutions have reported that useful lifespans can be longer than three years when training is very intense.
Evaluating Suppliers and Support Services
A supplier's dependability affects long-term happiness in addition to the product itself. Companies that have been making medical simulations for a long time know what is needed for healthcare teaching. Look for providers that offer full technical support, such as training on how to use the simulator most effectively, help with fixing problems, and advice on how to create a program.
Lead time and shipping logistics can change project timelines, especially for organizations that need to set exact dates for the start of training programs. Our normal production cycle gets custom-configured models to customers within 7–10 business days. We ship internationally with FedEx, DHL, and UPS, all of which are well-known carriers. Because of this responsiveness, training programs can keep going without long pauses.
Flexible payment options and clear prices help build trust between vendors and buyers. We take bank transfers and work directly with institutional purchasing offices to make the buying process easier. We are committed to honest business practices, which is why there are no secret design fees for requests for customization.
Technical Insights: Operation, Maintenance, and Training Curriculum
Maximizing return on investment from simulation equipment requires thoughtful integration into existing educational frameworks. The technology itself represents just one component of an effective training ecosystem.
Setup and Operational Best Practices
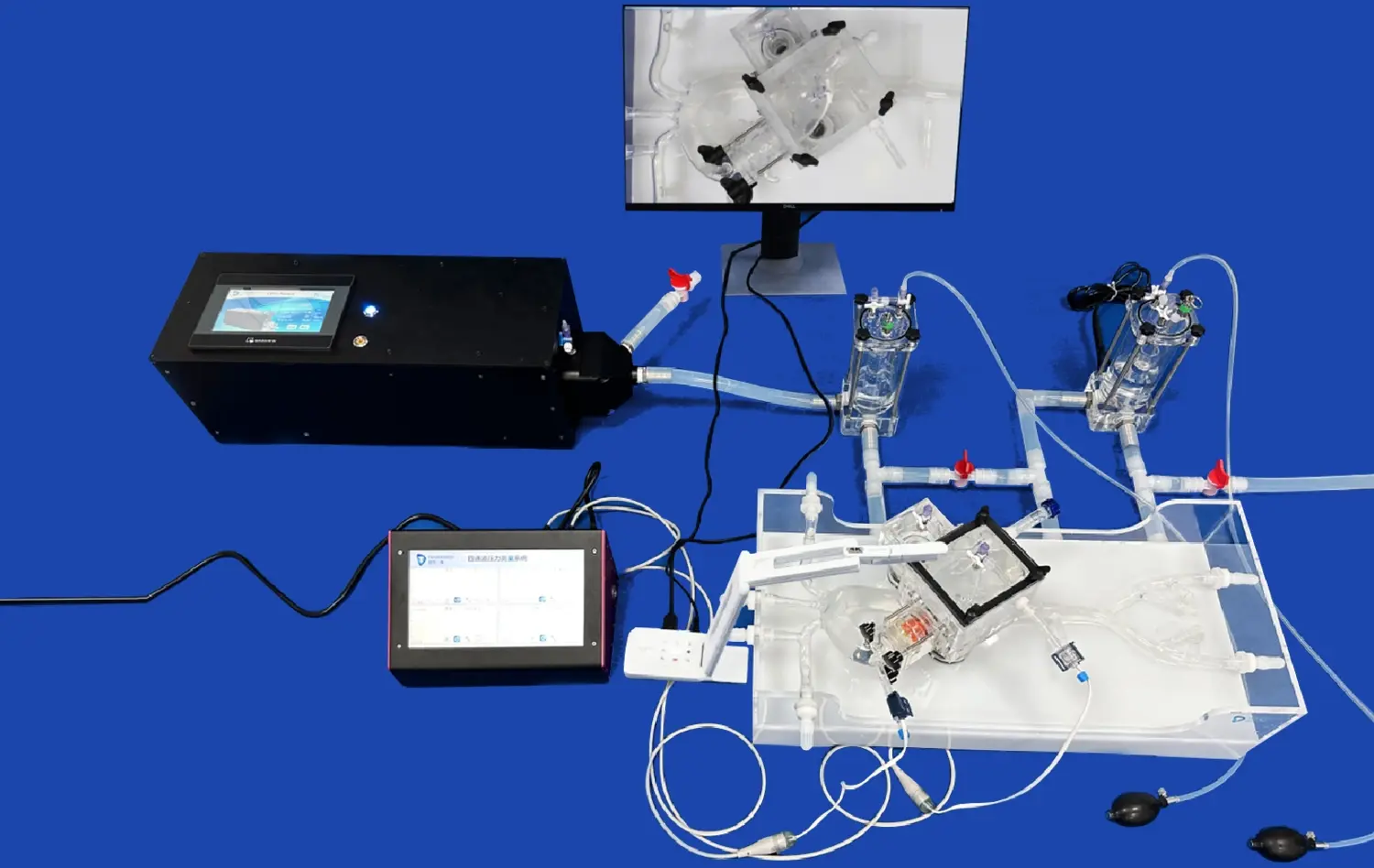
Proper simulator setup optimizes the training experience. The XXS003 congenital heart disease intervention training model connects to standard catheterization lab equipment, allowing trainees to use the same fluoroscopy systems, contrast injection tools, and monitoring displays they'll encounter clinically. This equipment compatibility reinforces the realistic training environment and avoids introducing artificial distinctions between simulation and practice.
Regular inspection routines extend simulator lifespan. After each training session, the vascular pathways should be flushed with clean water to remove residual contrast media or other materials. Visual inspection for tears or material degradation helps identify maintenance needs before they impact training quality. Storage in climate-controlled environments away from direct sunlight prevents premature material aging.
Curriculum Development for Maximum Learning Impact
Integrating simulators into structured educational pathways yields better outcomes than ad-hoc practice sessions. A progressive curriculum might begin with basic catheter navigation exercises, advance to guidewire manipulation and crossing techniques, then culminate in complete device deployment scenarios with varying defect anatomies.
Assessment metrics embedded in training protocols provide objective competency measurements. Tracking parameters like procedural completion time, fluoroscopy duration, contrast volume usage, and successful device positioning allows program directors to identify knowledge gaps and tailor additional instruction accordingly. This data-driven approach to skills development mirrors the quality improvement methodologies increasingly adopted throughout healthcare.
Simulation training proves particularly valuable when introducing new device technologies. As manufacturers innovate occlusion devices with novel deployment mechanisms or sizing characteristics, simulation provides safe environments for experienced operators to develop familiarity before clinical application. This continuing education application extends the simulator's value beyond initial training purposes.
Measuring Effectiveness and Research on ASD Occlusion Training Models
The medical education community increasingly demands evidence supporting educational interventions. Simulation-based training has accumulated substantial research validation demonstrating measurable improvements in procedural performance.
Clinical Evidence Supporting Simulation Training
Multi-center studies examining interventional cardiology training outcomes consistently show that simulation exposure correlates with improved clinical metrics. A 2021 investigation involving eight academic medical centers found that fellows who completed standardized ASD occlusion simulator training achieved device deployment success rates 23% higher than control groups during their initial twenty clinical cases. The simulator-trained group also demonstrated 31% shorter procedure times and 28% lower radiation exposure.
Performance improvements extend beyond technical execution to include better decision-making under pressure. Simulator training that incorporates complications—such as device malposition, wire entanglement, or hemodynamic instability—prepares operators to recognize and manage adverse events. This cognitive preparation enhances patient safety by reducing panic responses when unexpected situations arise.
Future Directions in Simulation Technology
Emerging technologies promise even more sophisticated training experiences. Virtual reality integration could overlay anatomical information or procedural guidance onto physical simulators, creating augmented training environments. Artificial intelligence algorithms might analyze operator technique in real-time, providing immediate feedback on catheter manipulation, device positioning, and efficiency.
Haptic feedback systems represent another frontier, offering the potential to simulate various tissue pathologies with adjustable resistance profiles. As these technologies mature and become cost-effective, training programs will gain unprecedented flexibility in scenario creation and skill assessment.
The trajectory clearly points toward simulation becoming standard practice throughout cardiovascular training, much as flight simulators became mandatory in aviation education decades ago. Institutions that invest in high-quality training infrastructure position themselves as leaders in clinical education and patient safety.
Conclusion
Simulation technology has fundamentally transformed congenital heart disease intervention training, offering safe, repeatable, and anatomically accurate platforms for skill development. The evidence supporting simulator-based education continues strengthening, with measurable improvements in procedural outcomes and trainee confidence. As healthcare institutions prioritize patient safety alongside educational excellence, high-fidelity congenital heart disease intervention training models become essential investments rather than optional enhancements. The combination of realistic anatomy, durable materials, and customization flexibility ensures these tools remain relevant throughout evolving clinical practices and device innovations.
FAQ
What distinguishes high-quality congenital heart simulators from basic models?
Superior simulators replicate complete vascular pathways with anatomically accurate dimensions and tissue-like compliance. The XXS003 model includes femoral access sites, iliac vessels, IVC, and both atrial chambers with customizable septal defects. Material properties matching human tissue provide realistic tactile feedback during catheter manipulation. Lower-quality alternatives often simplify anatomy or use materials with unrealistic mechanical characteristics, limiting training transfer to clinical settings.
How frequently do these simulators require maintenance or replacement?
Routine maintenance involves post-session cleaning and periodic visual inspections for material integrity. With proper care, silicone-based models maintain functionality through several hundred practice procedures. Replacement needs depend on usage intensity and storage conditions. Institutions typically plan for three-to-five-year replacement cycles under regular training program use.
Can simulators be customized for specific patient anatomies or rare defect presentations?
Customization represents a significant advantage of modern 3D printing manufacturing. We create patient-specific models from CT or MRI imaging data, allowing surgical teams to rehearse complex cases before entering the operating room. Defect sizes, locations, and associated anatomical variations can all be tailored to match educational objectives or specific clinical scenarios.
Partner With Trandomed for Advanced Cardiac Simulation Solutions
Trandomed specializes in developing anatomically precise congenital heart disease intervention training models that elevate clinical education standards. As a leading manufacturer in medical 3D printing technology, we combine over two decades of innovation with responsive customer service tailored to institutional procurement needs. Our XXS003 ASD occlusion simulator delivers the anatomical fidelity, material realism, and customization flexibility that training programs demand. Whether equipping a new simulation center, upgrading existing curriculum tools, or preparing teams for complex patient cases, our engineering team provides personalized solutions without additional design fees. Contact jackson.chen@trandomed.com to discuss your specific training requirements, request product demonstrations, or obtain institutional pricing information. Discover why leading medical schools and hospital training departments trust Trandomed as their congenital heart disease intervention training model supplier.
References
Barsness KA, Rooney DM, Davis LM. Collaboration in simulation: the development and initial validation of a novel thoracoscopic neonatal simulator. Journal of Pediatric Surgery. 2013;48(6):1232-1238.
Fann JI, Caffarelli AD, Georgette G, et al. Improvement in surgical performance using simulation-based training: a randomized trial. Annals of Thoracic Surgery. 2014;98(1):170-176.
Feins RH, Burkhart HM, Conte JV, et al. Simulation-based training in cardiac surgery. Journal of Thoracic and Cardiovascular Surgery. 2017;153(5):1233-1238.
Olivieri L, Krieger A, Loke YH, et al. Three-dimensional printing of intracardiac defects from three-dimensional echocardiographic images: feasibility and relative accuracy. Journal of the American Society of Echocardiography. 2015;28(4):392-397.
Pushparajah K, Barlow A, Tran VH, et al. A systematic review of the accuracy of cardiovascular magnetic resonance imaging for planning transcatheter structural interventions. International Journal of Cardiology. 2013;167(6):2453-2461.
Vukicevic M, Mosadegh B, Min JK, Little SH. Cardiac 3D printing and its future directions. JACC Cardiovascular Imaging. 2017;10(2):171-184.