Cerebral model technology has changed neurovascular training by making structural copies that are very close to the real thing. This lets students practice procedures without putting patients at risk. These 3D-printed models make accurate copies of complicated blood vessel structures like aneurysms and artery routes. This lets doctors improve their skills in safe settings. These training tools make a big difference in clinical skill and patient safety across medical schools, hospitals, research labs, and practice centers across the country by connecting theory knowledge with real-world application.
Understanding Cerebral Vascular Simulators and Their Role in Neurovascular Training
Neurovascular training needs accuracy in anatomy, precision, and lots of chances to practice, which is hard to get with standard methods. Our cerebral vascular models solve these problems by giving doctors accurate copies of the arteries and veins in the brain that they can use over and over again without having to worry about ethics or lack of resources.
What Makes Modern Neurovascular Simulators Different
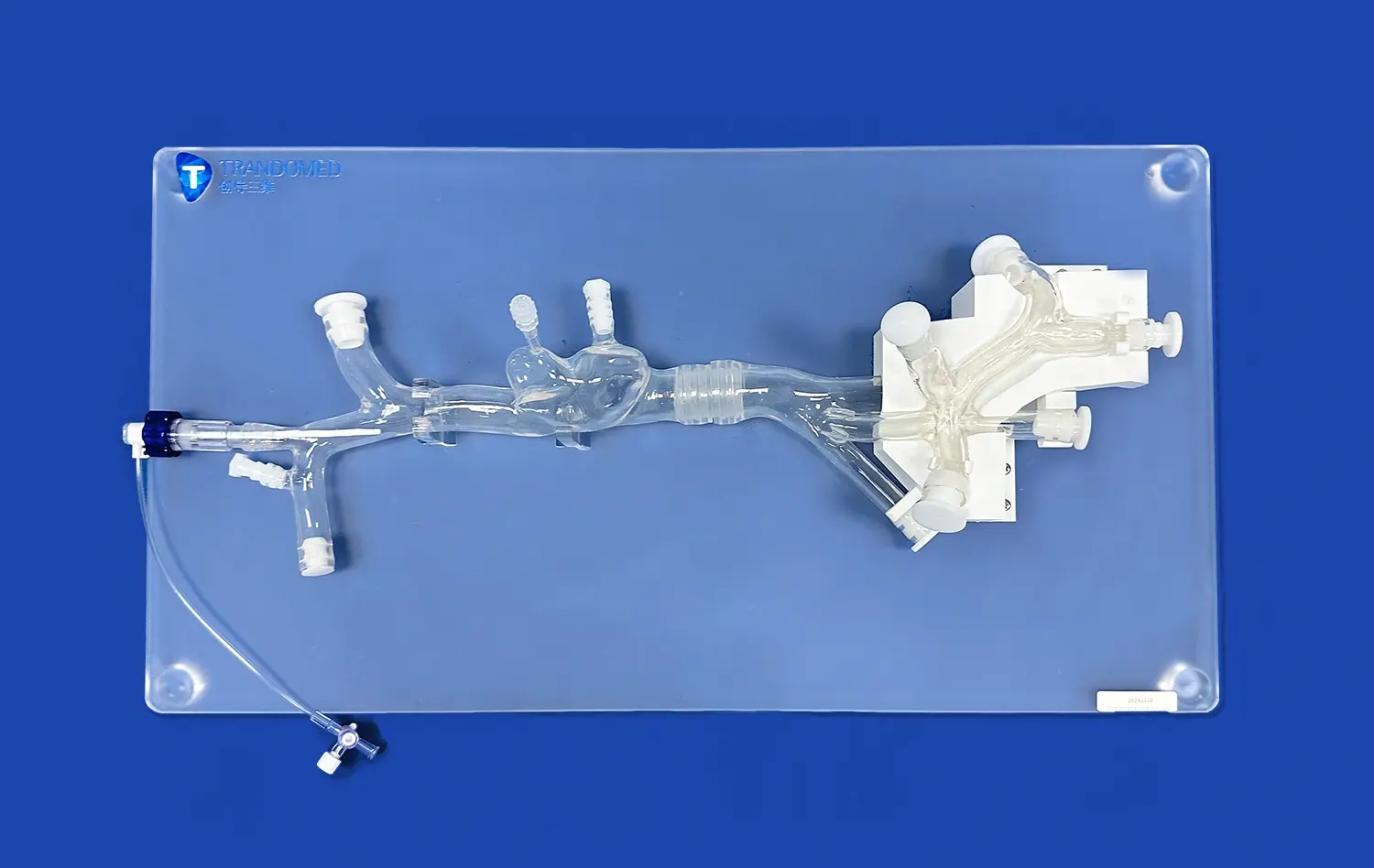
The Circle of Willis Aneurysm III (Product No. SJK002D) is a big step forward in the technology used to simulate the human body. This device, which is made of medical-grade Silicone Shore 40A, accurately models the brain arteries. During surgical operations, the choice of material gives accurate physical feedback during catheter guidance, making it feel like you are touching real blood vessels.
The model includes a number of different aneurysm sites, such as the eye section, the basilar artery, the carotid artery, and the middle cerebral artery. This variety lets trainees experience different clinical situations on the same training setting. When put in the plastic box that comes with it, the three-dimensional links between spaces are immediately clear. This helps students develop the mental mapping skills that are needed for treatments to work.
Applications Across Medical Education and Clinical Practice
These models are used in medical and nursing schools to teach vascular anatomy in ways that learning from cadavers can't. Students can practice inserting catheters, getting guidewires through blood vessels that are twisted, and coiling aneurysms over and over again until their muscles get used to the movements. Being able to make mistakes without getting in trouble makes for a mentally safe learning setting that helps people learn faster.
During meetings for planning before surgery, these models help hospitals and medical training units. Using modified versions made just for each patient, surgeons can practice difficult operations and find problems before they go into the operating room. This planning cuts down on the time needed for surgery, lowers the risk of problems, and improves patient results. All of these things have a direct effect on hospital performance measures and patient happiness scores.
These anatomy models are used by research centers to test and validate devices. Medical device companies that are making new stents, microcatheters, or embolic materials need testing systems that are as close to real human flesh as possible. Our sims offer uniform, repeatable testing settings that shorten the time it takes to make new products and cut down on the use of animal models.
Customization Capabilities for Specialized Training Needs
We know that different schools have different problems with teaching. With our customization services, you can tell us exactly how many aneurysms you need, how big they are, and where they are in the body so that they meet the needs of your program or study methods. Aside from aneurysms, we can also include stenosis at different levels of severity, vessel tortuosity, embolic formations, and other abnormalities that trainers need to be able to spot and handle.
Medical image data in CT, CAD, STL, STP, and STEP files can be used in the customizing process for a cerebral model. Because of this similarity, you can use real clinical cases to make models that are special to each patient. This turns real-life situations into training tools that can be used again and again. The whole process, from sending in the data to getting the model back, usually only takes 7–10 days, and there are no design fees for making changes. This quick turn-around helps study projects that need to be finished quickly and lets school programs quickly update their training catalogs as their courses change.
Advantages of Physical Simulation Models Over Traditional Neurovascular Training Methods
In the past, neurovascular training mostly consisted of watching, reading, and having a few hands-on sessions with supervising doctors. Even though these methods are useful, they have major flaws that can be fixed with current modeling technology.
Overcoming the Limitations of Conventional Training Approaches
Even though cadaver-based training is physically accurate, it is hard to get, the tissues break down, and there are ethical concerns. Specimens can't be used over and over again, which puts pressure on costs and schedules. Concerns about ethics come up when using animal models to study human vascular structure, especially the unique features of brain circulation.
Real experience is gained by doing treatments on real patients while being supervised, but patient safety is always put ahead of learning efficiency. Trainees can't easily try out different methods or fix mistakes, which limits the depth of learning through experience. Working with real patients can also make you more anxious, which, as study has shown, makes it harder to learn new skills in the beginning.
Quantifiable Benefits in Training Outcomes and Safety
Studies in the books on neurosurgical training show that training through simulations greatly lowers the number of mistakes that happen during the first real patient cases. Residents who trained with physical vascular models did 40% fewer guidance mistakes and finished procedures 30% faster than their peers who only did standard training.
These improvements translate directly to patient safety. Fewer problems mean that patients stay in the hospital for less time, pay less, and have better results. When organizations spend money on high-fidelity simulation training, they're also lowering risk, which is a goal shared by hospital managers, quality improvement groups, and lawsuit insurance.
The repeatability advantage cannot be overstated. A single arterial model can be used over and over again without breaking down, so whole groups of students can have the same training experiences. This regulation makes sure that competency tests measure real skill and not differences in the quality of training opportunities.
Real-World Implementation Success Stories
Our arterial models are used in neurosurgery and interventional radiology courses at a number of well-known medical schools. Faculty say that by the time students do their first guided treatments on a patient, they have gained confidence and simple technical skills that used to take months to build. Because of this speeding up, training programs can cover more advanced methods in the same amount of time, which means that grads are better prepared for their careers.
For ongoing medical education programs, these models such as the cerebral model are used in surgical training labs at specialty hospitals. This helps experienced doctors learn new skills as invasive methods change. Being able to try out new techniques in a safe setting before doing them on patients helps with both professional legal issues and ethical duties to stay up to date on skills.
Selecting the Right Neurovascular Training Simulator for Your Institution
When deciding what medical training tools to buy, it's important to think about more than just the original cost. Investing in the right simulator will pay off because it will last, be flexible, allow for customization, and come with ongoing support.
Critical Evaluation Criteria for Procurement Teams
Anatomical precision is the most important thing that needs to be done. The model needs to accurately mimic the size of the vessels, the thickness of the walls, the curves of the branches, and the relationships between spaces so that skills can be regularly applied to patient care. The qualities of the materials are just as important—the response you feel when you move the tube around should be the same as the tissue's stiffness and flexibility.
Durability has a direct effect on value over time. When training programs use simulations a lot, they need models that don't break down and keep their true handling properties after hundreds of uses. Our Silicone Shore 40A material mixture is especially designed to meet this need. It doesn't break down when the tube goes through it multiple times and keeps its functional qualities.
Whether a single model can meet more than one training goal or whether institutions need to buy separate units for each situation depends on how flexible the customization is. Because you can choose the area and type of disease, one adjustable platform can replace several fixed-configuration options, which saves money.
Logistical Considerations for Institutional Adoption
Lead time affects how programs are planned, especially when new courses are introduced or training is made more extensive. Our production timeline of 7–10 days from order confirmation to delivery lets us be flexible with purchasing so that we can work with training and school plans. International shipping through FedEx, DHL, EMS, UPS, and TNT ensures safe arrival and tracking, which is what buying offices need.
For big sellers who have to deal with complicated approval processes, payment terms and procedures are important. We accept standard T/T payment plans that work with how institutions buy things, which makes the buying process easier and lowers the amount of paperwork that needs to be done.
The benefit of support and advice services goes beyond the product itself. Our team can help you figure out the best way to train, fix problems, and make suggestions for skill-building programs that build on each other. This helpful method helps institutions get the most out of their investments in simulations.
Building Long-Term Training Platform Partnerships
Instead of taking each buy as a one-time thing, educational schools and healthcare systems would be better off building long-term ties with simulation vendors. Keeping training lists up to date is easier when you have a partner who knows your program's past and goals and can adapt to changing training needs and new procedures.
We keep thorough records of all the changes that have been made in the past for a cerebral model. This lets us make quick reorderings or small changes as programs grow. This institutional memory cuts down on the time training leaders need to plan and makes sure that everything is the same when new units are added or programs are expanded.
Integrating Vascular Simulation into Comprehensive Neurovascular Training Workflows
For simulation-based training to work, it's not enough to just give people access to models. The best results in education come from incorporating it into organized courses with clear learning goals, growth paths, and skill evaluations.
Designing Progressive Skill Development Programs
Training programs that work slowly add more complicated steps, building basic skills first before moving on to harder situations. In the first classes, the focus might be on basic catheter travel through normal tissue. This would help students learn how to control the guidewire and understand how the arteries connect in three dimensions. These basic events give you the basic skills you need to do more difficult jobs.
Pathological changes like minor tortuosity, moderate stenosis, or easy-to-reach aneurysm sites are introduced in intermediate training. Learners get practice changing their skills to different body types while still working in situations that aren't too harsh. This gradual task keeps beginners from getting frustrated and losing their skills when they face too much difficulty too soon.
Advanced cases simulate the hardest clinical situations, like aneurysms in hard-to-reach places, severely tortuous vessels, or hardened stenosis. At this point, trainees have learned enough about these procedures to be able to try them with a good chance of success. This means that the difficulties are more likely to teach them than to discourage them. Because simulations are psychologically safe, they let students push their limits and learn how to solve problems without putting patients at risk.
Assessment and Competency Validation Methods
To do an objective review of ability, you need standard metrics that measure both technical skill and clinical sense. Time it takes to finish a procedure is one way to measure it, but it needs to be weighed against the quality of the technique—rushing through steps hurts learning. Tracking mistakes during treatments shows where specific skills are needed, like controlling a tube, manipulating a guidewire, or putting in a device.
Video recording lets you look back at your work and evaluate yourself in great detail. When trainees watch themselves do tasks, they become more aware of their technical habits, both the ones that help them and the ones that hurt them. This habit of reflecting speeds up change more than just getting feedback from others.
Simulation-based tests can help students get ready for guided treatments on real patients. Setting basic standards for skill on models before letting people into the operating room makes sure that everyone is safe at the start and gives clear factors that make progress decisions less subjective.
Emerging Applications and Future Directions
The next step forward in modeling training is the combination of monitoring technology and digital tracking systems. Models with pressure sensors, position tracking, and force measurement can give numeric feedback on how to manipulate a catheter, pointing out when too much force is being used or when the approach angle is not right. This data-driven input goes along with the usual observation by the teacher.
The use of virtual reality is another potential direction. Real-time fluoroscopic simulation that mimics the whole treatment experience could be made possible by combining actual vascular models with enhanced vision. Through hands-on experience, trainees would learn both the manual skills they need for processes and the skills they need to understand images.
Modeling apps that are tailored to each patient keep growing. The ability to make personalized practice models for complicated cases gets better as image and 3D printing technologies get better. This app is especially helpful for rare or odd diseases where surgeons may not have a lot of experience, as it lets them fully prepare before they face the real clinical situation.
Conclusion
Neurovascular training has changed a lot since high-fidelity tissue models such as the cerebral model were added. These simulators make practicing complicated techniques safe and repeatable. There are some major problems with the way training is usually done that these physical models fix. They also make trainees more competent and patients safer. As simulation-based learning becomes even more important in medical education, schools that spend money on good training tools put their programs at the top of the field when it comes to clinical education. When you put together physical correctness, realistic materials, the ability to customize, and a wide range of support services, you get training environments that make professionals who are ready for the difficulties of modern neurovascular care feel confident and skilled.
FAQ
What's the difference between virtual reality modeling and actual brain artery models?
Realistic material qualities and feedback that you can feel in physical models are things that current virtual reality systems can't fully copy. The reluctance you feel when moving the catheter, the flexibility of the vessel walls, and the three-dimensional spatial relationships you experience when manipulating things in real life are better at building muscle memory and procedural sense than simulators that only show what you're doing. Virtual systems are used to teach step-by-step procedures, and real models are used to build hands-on technical skills in many classes.
Can these models be used for teaching that is specific to an institution?
Of course. Our customization services let you choose the position, size, tortuosity, stenosis severity, and other clinical traits of aneurysms based on the needs of your program. Using CT scan data to make models that are specific to each patient lets doctors practice real procedures that are coming up. This gives you more control over the model, so it can meet your exact educational goals instead of pushing your program to fit into standard setups.
How long do you think these teaching models will last if they are used regularly?
When used according to the instructions, the Silicone Shore 40A material keeps its shape and realistic handling properties after hundreds of catheter runs. The actual length varies on how often it is used and how hard the procedures are, but most schools say that regular training classes for 12 to 18 months are enough to get good results. Despite possibly higher starting costs, the sturdiness is much better than options made from less durable materials, giving better long-term value.
How quickly can models that are made just for you be made and sent to you?
The normal time for production is between 7 and 10 days after the order is confirmed and the data file is received. Depending on the location and the time it takes to clear customs, international shipping can add an extra 3 to 5 days. For pressing needs, we may be able to do rush production. Please call our team to talk about your specific schedule needs. This quick turn-around helps curriculums adapt to new needs and lets training supplies be replaced on time as programs grow.
Do you offer teaching on the best ways to put educational plans into action?
We provide advice on topics such as creating lesson plans, ensuring students' skills improve over time, and figuring out how well they've learned new skills. Some people on our team have taught medical students before, so they know both how to use modeling tools technically and how to teach in a way that helps students learn the most. This advice helps schools avoid common execution mistakes so they can get more out of their training programs faster.
Partner with a Leading Cerebral Model Manufacturer for Superior Training Outcomes
Trandomed has 20 years of experience with medical modeling technology that can help you reach your goals for neurovascular training. Our Circle of Willis Aneurysm III model combines accurate anatomy with realistic materials and the ability to be customized in a wide range of ways. This makes training sessions that really prepare professionals for clinical challenges. Our full range of support services ensures that your training programs are set up correctly and are always being improved. Our team is ready to provide solutions that are tailored to your needs, whether you're creating new training programs, growing current ones, or looking for patient-specific practice models for difficult cases. Get in touch with jackson.chen@trandomed.com right away to talk about your neurovascular training needs, get full product specs, or set up test units to try out. As a company that supplies cerebral models and wants to improve medical education, we care about your success and the better results for patients that well-trained doctors provide.
References
Mashiko T, Konno T, Kawai R, Kaneko N, Otani K, Watanabe E. (2015). "Training in Cerebral Aneurysm Clipping Using Self-Made 3-Dimensional Models." Journal of Surgical Education, 72(4), 610-617.
Anderson JR, Thompson WL, Alkattan AK, Diaz O, Klucznik R, Zhang YJ, Britz GW, Grossman RG, Karmonik C. (2016). "Three-Dimensional Printing of Anatomically Accurate, Patient Specific Intracranial Aneurysm Models." Journal of NeuroInterventional Surgery, 8(5), 517-520.
Ryan JR, Chen T, Nakaji P, Frakes DH, Gonzalez LF. (2015). "Ventriculostomy Simulation Using Patient-Specific Ventricular Anatomy, 3D Printing, and Hydrogel Casting." World Neurosurgery, 84(5), 1333-1339.
Waran V, Narayanan V, Karuppiah R, Owen SL, Aziz T. (2014). "Utility of Multimaterial 3D Printers in Creating Models with Pathological Entities to Enhance the Training Experience of Neurosurgeons." Journal of Neurosurgery, 120(2), 489-492.
Kimura T, Morita A, Nishimura K, Aiyama H, Itoh H, Fukaya S, Sora S, Ochiai C. (2009). "Simulation of and Training for Cerebral Aneurysm Clipping with 3-Dimensional Models." Neurosurgery, 65(4), 719-726.
Mashiko T, Otani K, Kawano R, Konno T, Kaneko N, Ito Y, Watanabe E. (2015). "Development of Three-Dimensional Hollow Elastic Model for Cerebral Aneurysm Clipping Simulation Enabling Rapid and Low Cost Production." World Neurosurgery, 83(3), 351-361.

_1732863962417.webp)