Choosing the Right Left Atrial Appendage Closure Simulator for Labs
2026-05-14 09:00:04
Choosing the right left atrial appendage closure simulator is a very important task for medical training labs, research organizations, and hospitals that want to improve the education of cardiovascular procedures. These high-tech training tools help cardiologists and electrophysiologists learn LAAO techniques without any risks. They bridge the gap between academic knowledge and clinical competence. Millions of people around the world have atrial fibrillation, and closing the left atrial appendage is now seen as an important way to avoid strokes. This means that realistic simulation training is more important than ever. The right simulator gives your team the technical know-how and trust they need before they work with real patients. This improves the safety and outcomes of procedures.
Understanding Left Atrial Appendage Closure Simulators: Features and Benefits
The field of LAAO training has changed a lot thanks to advances in technology that have made it possible to use different types of simulations to meet different teaching goals.
Defining the Purpose of LAAO Simulation
In people with atrial fibrillation, the left atrial appendage forms a small pouch in the upper left chamber of the heart. This is a frequent place for blood clots to form. About 90% of the clots that cause strokes in people with AFib come from this part. Left atrial appendage closure procedures block this area so that clots can't get into the bloodstream. They can be used instead of long-term anticoagulation medicine. This anatomical environment is recreated in training models so that doctors can practice the careful catheter navigation, transseptal puncture, and device deployment that are needed for good results.
Types of Simulation Technologies Available
Modern training programs can pick from different types of simulators, each with its own benefits. Medical-grade plastic is used to make anatomical models that feel real in a way that virtual systems can't. Trainees can use these physical models to improve their hand-eye coordination and muscle memory, which are both important for manipulating catheters. Virtual reality platforms let you practice in an infinite number of situations for free, but they might not have the haptic feedback that is needed to feel tissue resistance. When you combine physical models with software tracking, you get full training experiences that keep track of performance metrics while keeping the true way tissues interact.
The Four LAA Morphologies and Training Implications
Finding four different forms for the left atrial appendage through research has huge implications for making simulators. In 48% of patients, the shape looks like a chicken wing, with a big bend that can make it harder to place a device correctly. Thirty percent of the time, cactus shapes have multiple lobes that need careful sizing measurement. Windsock variants, which are found in 19% of patients, only go in one main way. The cauliflower type is the rarest (only 3% of all types), but it has the most complicated anatomy, with uneven, multilobular shapes. Comprehensive training requires students to learn about all four shapes. This prepares them for the wide range of body types they will see in clinical practice.
Evaluating Simulator Options: What Labs Should Consider Before Buying?
To make an informed choice about what to buy, you need to carefully consider how the different features of the left atrial appendage closure simulator fit with your institution's training goals and operational limitations.
Anatomical Accuracy and Replicability
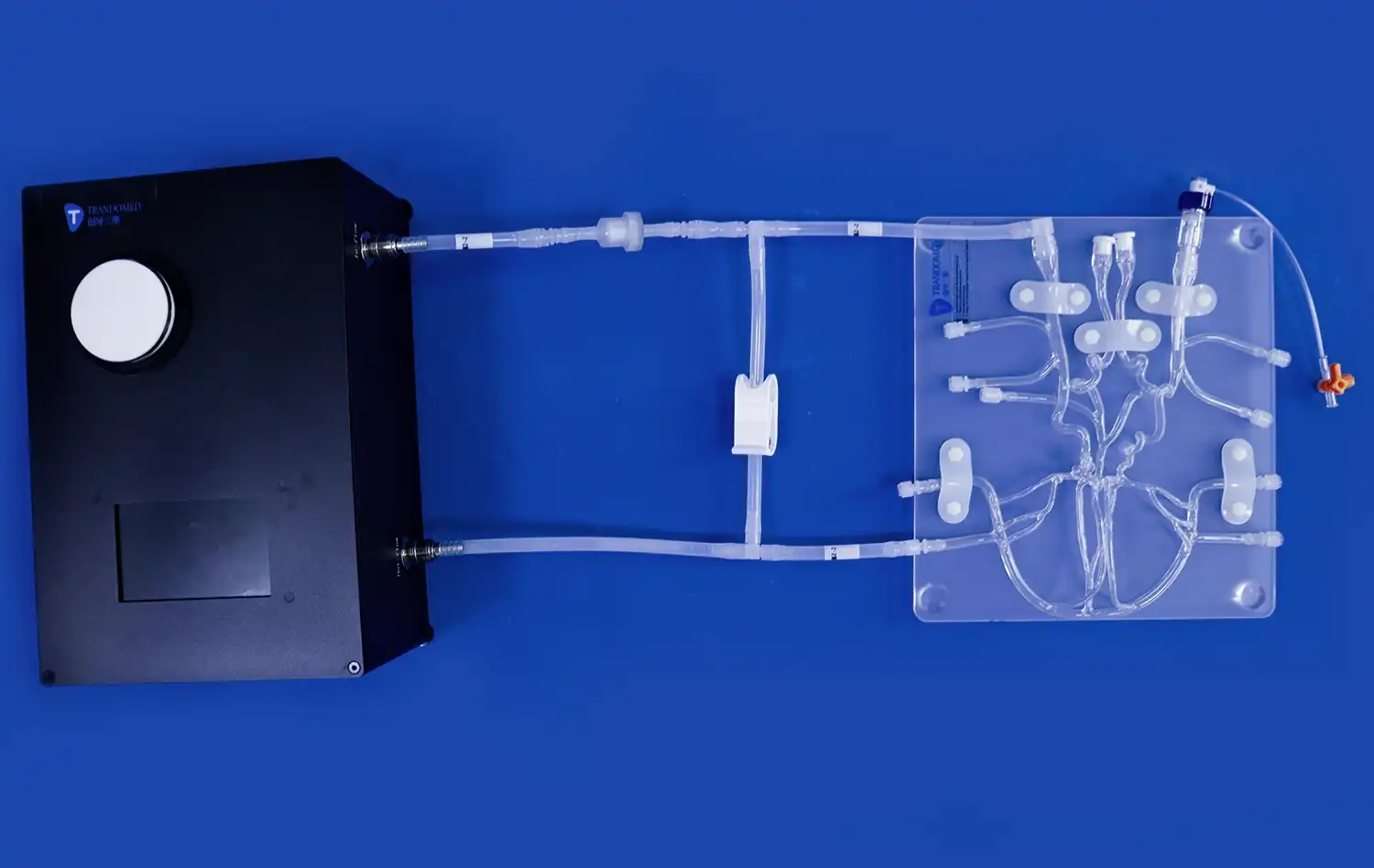
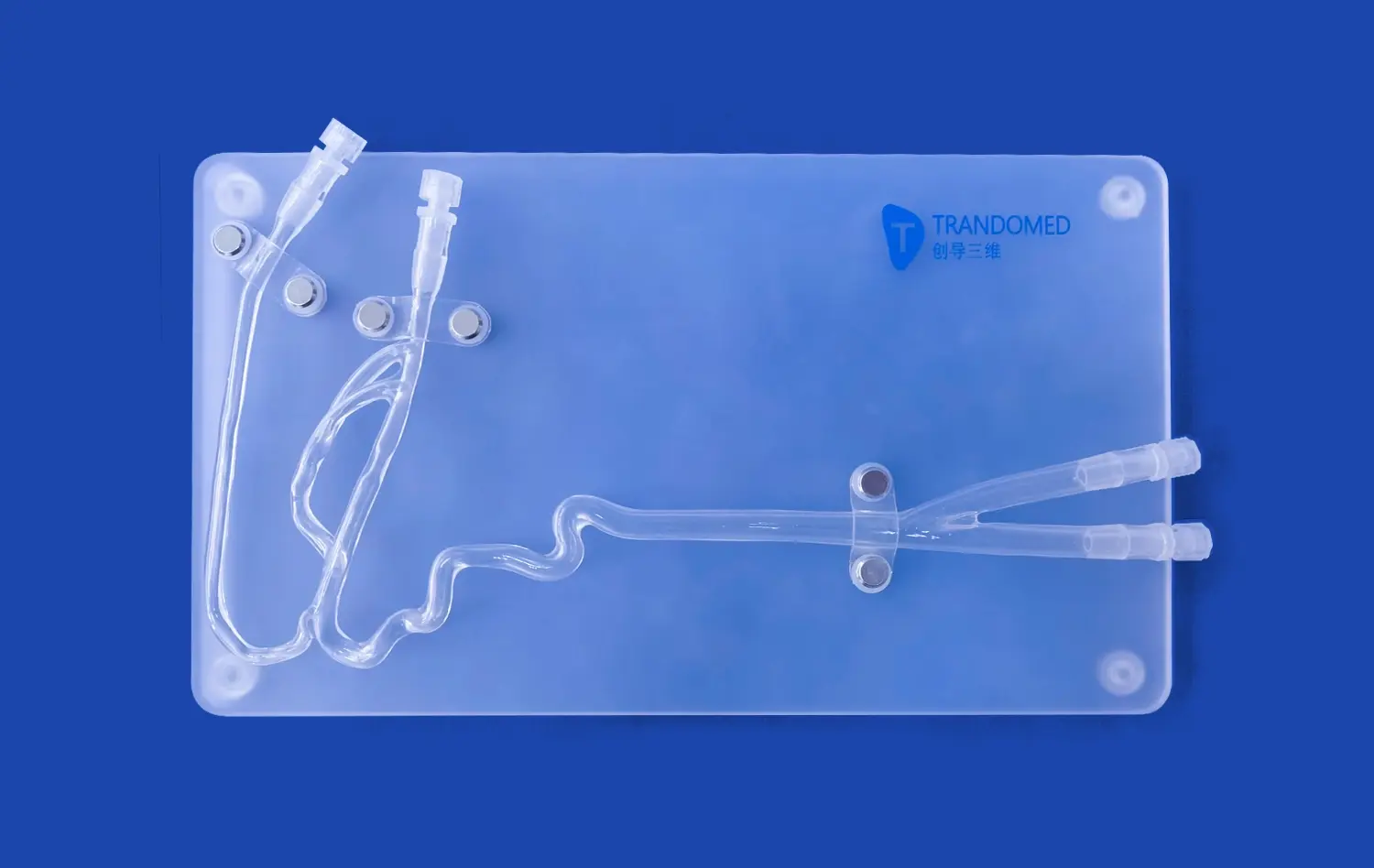
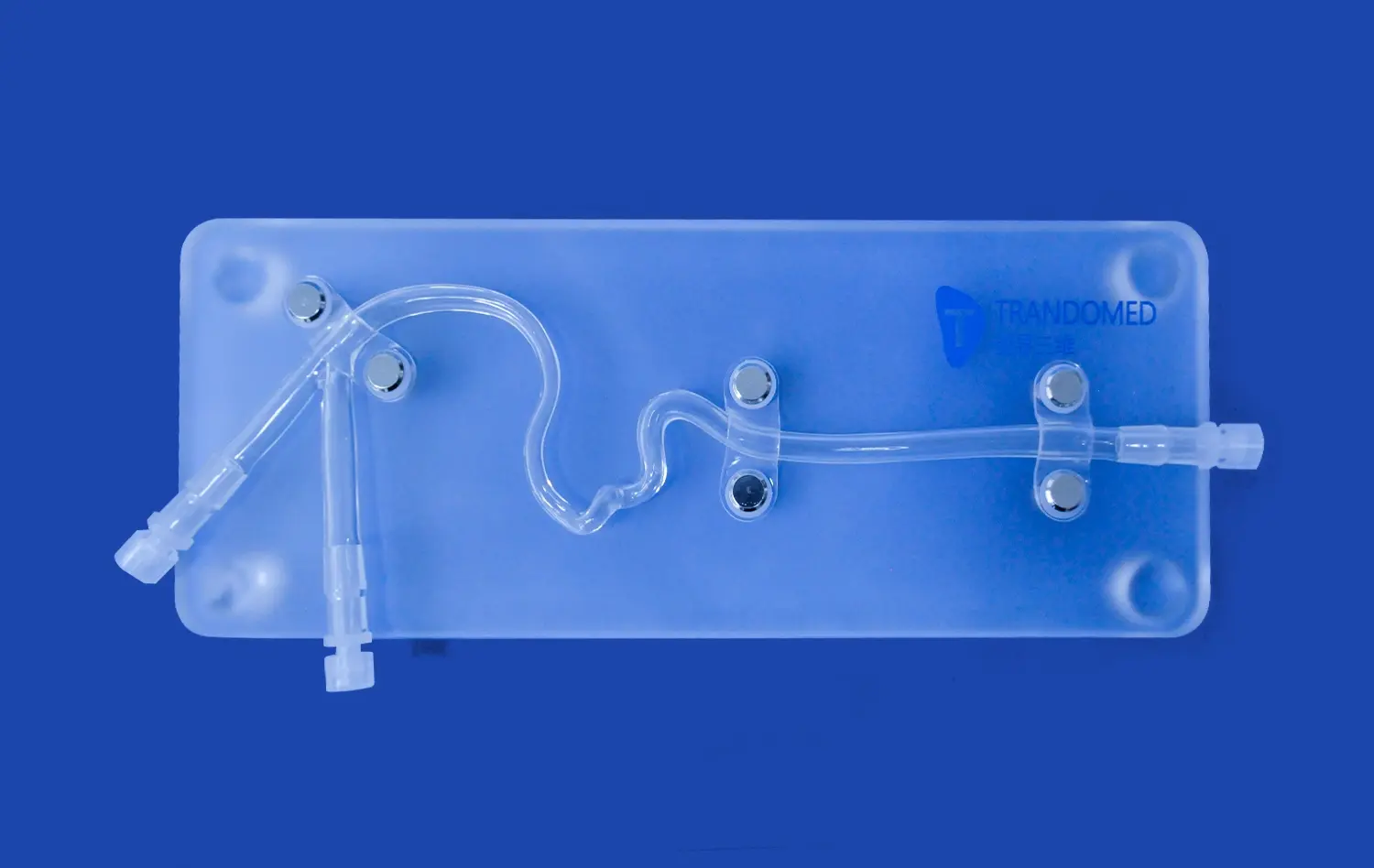
Anatomical accuracy is the key to successfully training with simulations. High-quality models show not only the left atrial appendage but also the whole procedure path from the femoral vein through the inferior vena cava, the right atrium, and the atrial septum. Look for simulators that correctly show the thickness of the vessel wall, the flexibility of the tissue, and the anatomical landmarks that are used to guide real procedures. The Trandomed XX013D model is a good example of this all-around method because it replicates the whole vascular path, from the femoral vein to the pulmonary veins, using medical-grade Silicone Shore 40A that acts like human tissue.
Modularity and Scenario Diversity
Getting used to different professional situations helps you get better at following procedures. Labs can get the most out of a single platform for teaching when the parts of the simulator can be switched out. Progressive skill growth is possible with models that show different LAA shapes and different atrial septal defect configurations. Trainees can start with simple anatomy cases and then move on to more difficult cases that are like problems that people face in the real world. Being able to practice transseptal puncture through different septal thicknesses and places helps you develop the flexibility you need to practice on your own.
Integration with Existing Training Infrastructure
Both short-term and long-term value are affected by how well the new tech works with the existing tools and processes in your lab. Instead of needing special training tools, physical models should be able to hold the catheters, guidewires, and closure devices that your team will actually use in the clinic. Check to see if the model can connect to your fluoroscopy or echocardiography simulation systems so that it can work like the multimodal imaging guiding that is used in real life. Integration that doesn't cause any problems makes setup easier and makes training more like being in a clinical setting.
Matching Simulator Features to Lab Needs: A Demand Matching Approach
To get the best educational return on investment, each school should choose a simulator based on its training population and goals.
Aligning Simulator Complexity with User Expertise Levels
Medical schools that teach students about interventional cardiology need different things than fellowship programs that train advanced practitioners. Beginners can start with clear models that show where the catheter is in relation to body structures. This helps them understand space before moving on to more complicated models that need imaging help. Advanced trainees need models that are accurate in terms of anatomy and that test their technical skills by showing real-life tissue qualities and problems that could happen. Because sophisticated simulators are made up of separate modules, schools can increase the level of difficulty as students improve their skills. This makes the investment last longer.
Customization Capabilities for Research Applications
Companies that make devices and do research have specific needs that go beyond normal training protocols. To be able to change the size of anatomical parts, make models that are specific to a patient from imaging data, or try prototype devices, customization needs to be very flexible. Trandomed can work with CT, CAD, STL, STP, and STEP file types, which lets you make models that are specific to your study questions or product development needs. Because it can be changed, the simulator can be used as both a teaching tool and a flexible research platform for validating devices, studying biomechanics, and improving procedures.
Budget Considerations and Total Cost of Ownership
The most obvious cost is the acquisition cost, but smart procurement professionals look at the total ownership cost, which includes replacement parts, maintenance needs, and ways to update. Durable construction with high-quality materials lowers the number of replacements needed, but the original cost may be higher. When compared to single-use disposable systems, models with replaceable parts in high-wear areas like atrial septal defects are more cost-effective over the long run. To properly compare options across a range of price points and levels of durability, you should figure out how much each training session will cost over the left atrial appendage closure simulator's expected lifetime.
Procurement Considerations: How to Buy and What to Expect?
Understanding the buying process helps institutions choose vendors, coordinate logistics, and plan for implementation so that the deployment of simulation skills goes smoothly.
Evaluating Manufacturers and Supplier Credentials
Working with a well-known company that has a lot of experience with research and development gives you peace of mind about the quality of the products and the fact that new ideas will keep coming up. Ningbo Trando 3D Medical Technology Co., Ltd has been a leader in China in this field for over 20 years by focusing on medical 3D printing technology. Their design process, which is based on real CT and MRI scans of people, ensures anatomical correctness that models that are only based on theory can't reach. Reverse 3D reconstruction technology pulls out exact anatomical details that are then optimized for educational success. This makes simulators that are both realistic and useful for training.
Understanding Lead Times and Shipping Logistics
When planning when to buy a simulator, you need to take into account both production schedules and shipping costs between countries. Production times are usually between one and two weeks, but they can be longer if you need custom setups. The XX013D model has a lead time of seven to ten days, which means that it can be sent out pretty quickly after your order is approved. International shipping through well-known companies like FedEx, DHL, or UPS guarantees safe arrival with tracking. However, institutions should be aware of the customs clearance process when bringing medical training equipment into the country.
Payment Terms and Customization Services
Financial arrangements and policies on tailoring have a big effect on the ability of institutions with complicated approval processes or specific training needs to buy things. Standard payment terms through bank transfer make transactions easy to handle, and open customization policies make it easy to get equipment that is exactly what you need. Trandomed's policy of letting customization happen without charging design fees gets rid of a big cost barrier. This means that institutions can get the best training solutions without having to pay engineering fees that break the bank. This method is based on a customer-focused philosophy that puts educational results ahead of making the most money per unit.
Ensuring Training Effectiveness and Measuring ROI with Your Simulator
Using simulation technology is only the beginning. To have the most educational effect, it needs to be implemented in a structured way and the results need to be evaluated.
Establishing Performance Metrics and Competency Benchmarks
Simulation training goes from being free practice to competency-based education with clear results when objective measurements are used. Set clear goals for each skill, like the amount of time needed to complete a successful transseptal puncture, the accuracy of placing the device in relation to the LAA ostium, and the speed at which complications are recognized. Track changes in performance over several practice sessions to keep track of skill learning curves and figure out which trainees need more help. These metrics help learners see their own growth, show proof to accreditation bodies, and show program administrators why they should spend money on the program.
Integrating Simulation into Comprehensive Training Curricula
If you want simulations to work best, you should carefully incorporate them into larger training programs instead of doing them on their own. Before using a simulator for practice, start with teaching lessons that go over the procedure's benefits and drawbacks and how to do it step by step. After hands-on training, there are debriefing meetings where teachers talk about performance, help students make decisions, and go over important ideas again. Trainees can only move from simulator practice to controlled clinical cases after they have shown they are consistently competent on all possible anatomical variations. This planned progression boosts trust while upholding safety standards for patients.
Future Trends Shaping Simulation Technology
As simulation technology keeps improving, it will be possible to have more complex training situations that will help teach procedures even better. Adding artificial intelligence will allow performance evaluations to be done automatically, giving instant feedback without the need for an instructor to be present at all times. Better haptic feedback systems will give you more complex tactile feelings, simulating the subtleties of tissue that are currently hard for simulation technology to do. Soon, augmented reality overlays might be able to cast anatomical information onto real-life models, combining the benefits of practicing with your own body with the huge amounts of data available in digital systems. Knowing about these changes helps institutions plan ways to improve their simulations that protect the money they have already spent on them.
Conclusion
Choosing the optimal left atrial appendage closure simulator demands careful consideration of anatomical fidelity, training objectives, institutional requirements, and long-term value. Physical models offering comprehensive vascular replication, multiple LAA morphologies, and modular components provide versatile platforms supporting diverse educational needs. Partnering with experienced manufacturers who understand medical education requirements and offer customization flexibility ensures your investment delivers sustained training effectiveness. The right simulator becomes more than equipment—it transforms into an essential educational partner that elevates clinical competency, enhances patient outcomes, and positions your institution at the forefront of cardiovascular procedural training.
FAQ
What is a left atrial appendage closure procedure?
Left atrial appendage closure represents a minimally invasive intervention that seals off the left atrial appendage to reduce stroke risk in patients with atrial fibrillation. During the procedure, cardiologists advance a catheter from the femoral vein through the heart's right side, puncture the atrial septum, and deploy a closure device within the LAA. This mechanical barrier prevents blood clots that form in the appendage from entering circulation and causing strokes, offering an alternative to lifelong anticoagulation therapy for patients who cannot tolerate blood thinners.
What are the four types of left atrial appendage morphologies?
Following extensive imaging studies of patient populations, researchers have classified four primary LAA shapes: chicken wing, cactus, windsock, and cauliflower. The chicken wing configuration, characterized by a pronounced bend, appears in approximately 48% of patients. Cactus morphologies with central body and secondary lobes occur in 30% of cases. Windsock variants featuring single-direction extension represent 19% of anatomies. The rarest cauliflower type, present in just 3% of patients, displays irregular multilobular structures that present unique procedural challenges.
How do physical simulators compare to virtual reality training systems?
Physical simulators provide tactile feedback and realistic tissue interaction that develops the fine motor skills essential for catheter manipulation, while virtual reality systems offer unlimited practice scenarios without consumable costs. Anatomical models excel at teaching device deployment techniques and building muscle memory through repeated hands-on practice with actual clinical equipment. Virtual platforms contribute value through performance tracking, immediate feedback, and exposure to rare complications without physical model limitations. Comprehensive training programs often incorporate both modalities to leverage their complementary strengths.
What customization options should labs consider when ordering simulators?
Customization capabilities transform standard simulators into precisely targeted educational tools. Consider requesting specific LAA morphologies matching your patient population demographics, variable atrial septal defect positions reflecting your procedural approach preferences, or patient-specific anatomies reconstructed from imaging data for pre-procedural planning. Labs engaged in device research should explore material property modifications or dimensional alterations that support product testing protocols. Manufacturers offering file format flexibility for CT, CAD, or STL data enable the broadest customization possibilities.
How can institutions measure training effectiveness with simulators?
Effective assessment combines objective performance metrics with subjective competency evaluations. Track quantitative measures including procedure completion time, fluoroscopy duration, number of catheter repositioning attempts, and device placement accuracy relative to anatomical landmarks. Supplement these metrics with structured competency checklists evaluating decision-making, complication recognition, and troubleshooting capabilities. Compare performance trends across multiple practice sessions to document skill progression, and establish minimum competency thresholds before authorizing independent clinical practice.
Get Started with Trandomed's Advanced LAAO Training Solutions
Trandomed stands ready to support your institution's commitment to excellence in cardiovascular procedural education. As a leading left atrial appendage closure simulator manufacturer, we combine two decades of 3D medical printing expertise with deep understanding of clinical training requirements. Our XX013D model delivers the anatomical precision, morphological diversity, and durability your program needs to build practitioner confidence and competency. Customization capabilities ensure the simulator aligns perfectly with your specific training protocols without additional design costs. Reach out to jackson.chen@trandomed.com to discuss your training objectives, explore customization options, and discover how our simulation technology can elevate your educational outcomes. Whether you're establishing a new training program or enhancing existing capabilities, our team provides the technical support and product expertise to ensure your success.
References
American College of Cardiology Foundation. (2021). Guidelines for Left Atrial Appendage Occlusion in Atrial Fibrillation: Evidence-Based Recommendations for Clinical Practice. Washington, DC: ACC Publications.
European Society of Cardiology Working Group on Cardiovascular Surgery. (2020). Simulation-Based Training in Interventional Cardiology: Standards and Best Practices for Medical Education Programs. Munich: ESC Educational Materials.
Journal of Medical Simulation and Healthcare Education. (2022). "Comparative Effectiveness of Physical Versus Virtual Reality Simulators in Left Atrial Appendage Closure Training: A Multi-Center Randomized Trial." Vol. 17, Issue 4, pp. 234-248.
Society for Cardiovascular Angiography and Interventions. (2021). Competency Guidelines for Left Atrial Appendage Closure Procedures: Training Requirements and Assessment Protocols. Washington, DC: SCAI Educational Resources.
Wang, D., Holmes, D. R., and Reddy, V. Y. (2019). Left Atrial Appendage Closure: Technical Considerations and Clinical Outcomes. Oxford: Blackwell Medical Publishing.
International Consortium for Medical Simulation Technology. (2023). Advancements in 3D-Printed Anatomical Models for Cardiovascular Procedural Training: Materials, Methods, and Clinical Applications. Boston: ICMST Academic Press.