How Congenital Heart Disease Training Models Improve ASD Skills?
2026-05-22 09:00:04
Procedures for atrial septal defect (ASD) need accuracy, trust, and a lot of hands-on experience. Cardiologists, pediatric doctors, and medical students can learn these difficult skills in a safe, realistic setting with a congenital heart disease intervention training model. Traditional methods depend on limited patient exposure. These simulation tools, on the other hand, mimic real cardiac anatomy, such as the femoral vein, iliac vein, inferior vena cava, and atrial chambers. This lets doctors improve catheter navigation, device deployment, and complication management without putting patients at risk. This method speeds up the learning of skills while also making patient outcomes better across all medical schools in the country.
Understanding Congenital Heart Disease Intervention Training Models
Modern simulation technology has changed the way doctors and nurses are trained to do complicated heart treatments. By showing congenital defects in a way that is true to life, these specialized tools bridge the gap between theoretical knowledge and clinical practice.
Anatomical Accuracy Drives Learning Outcomes
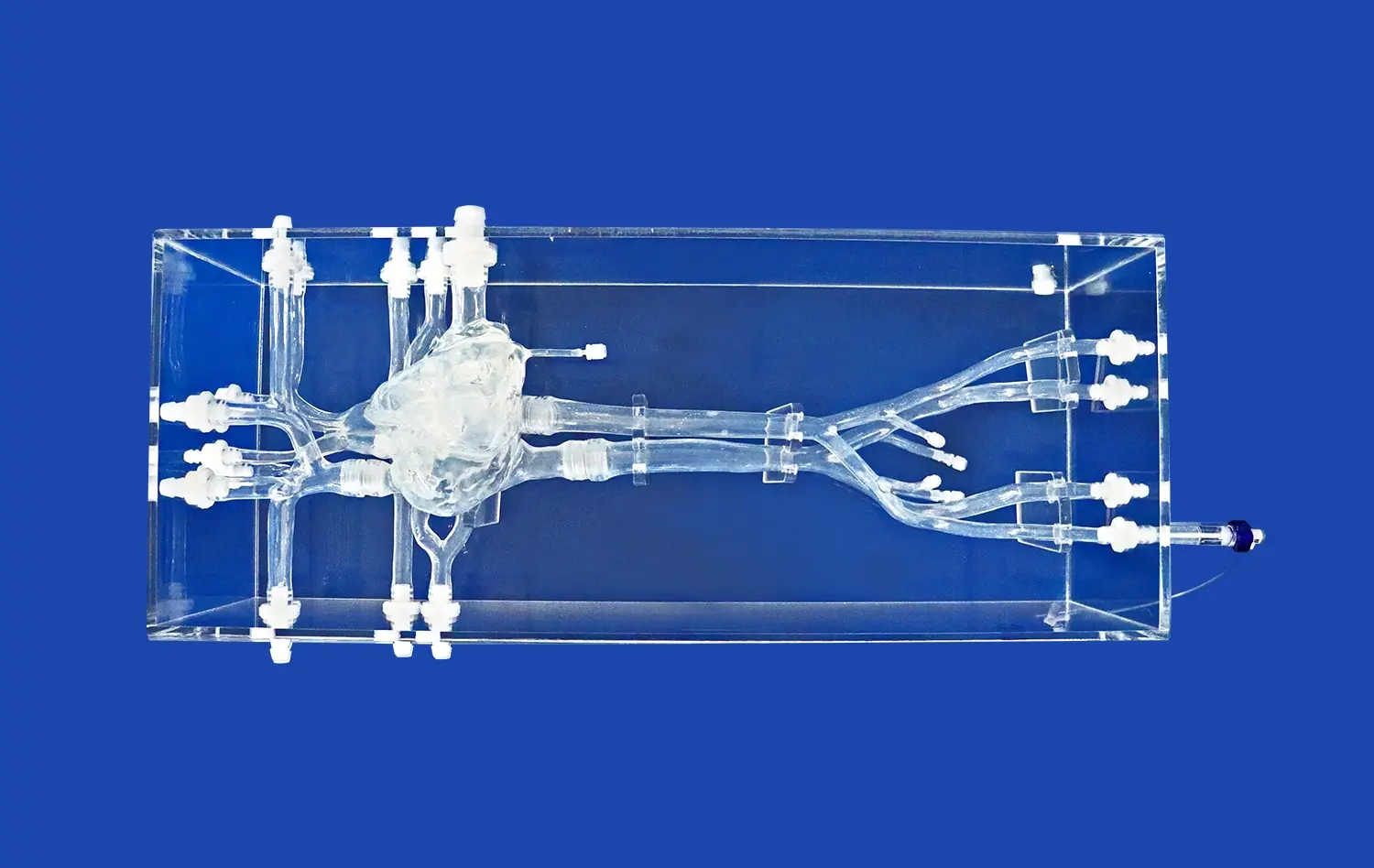
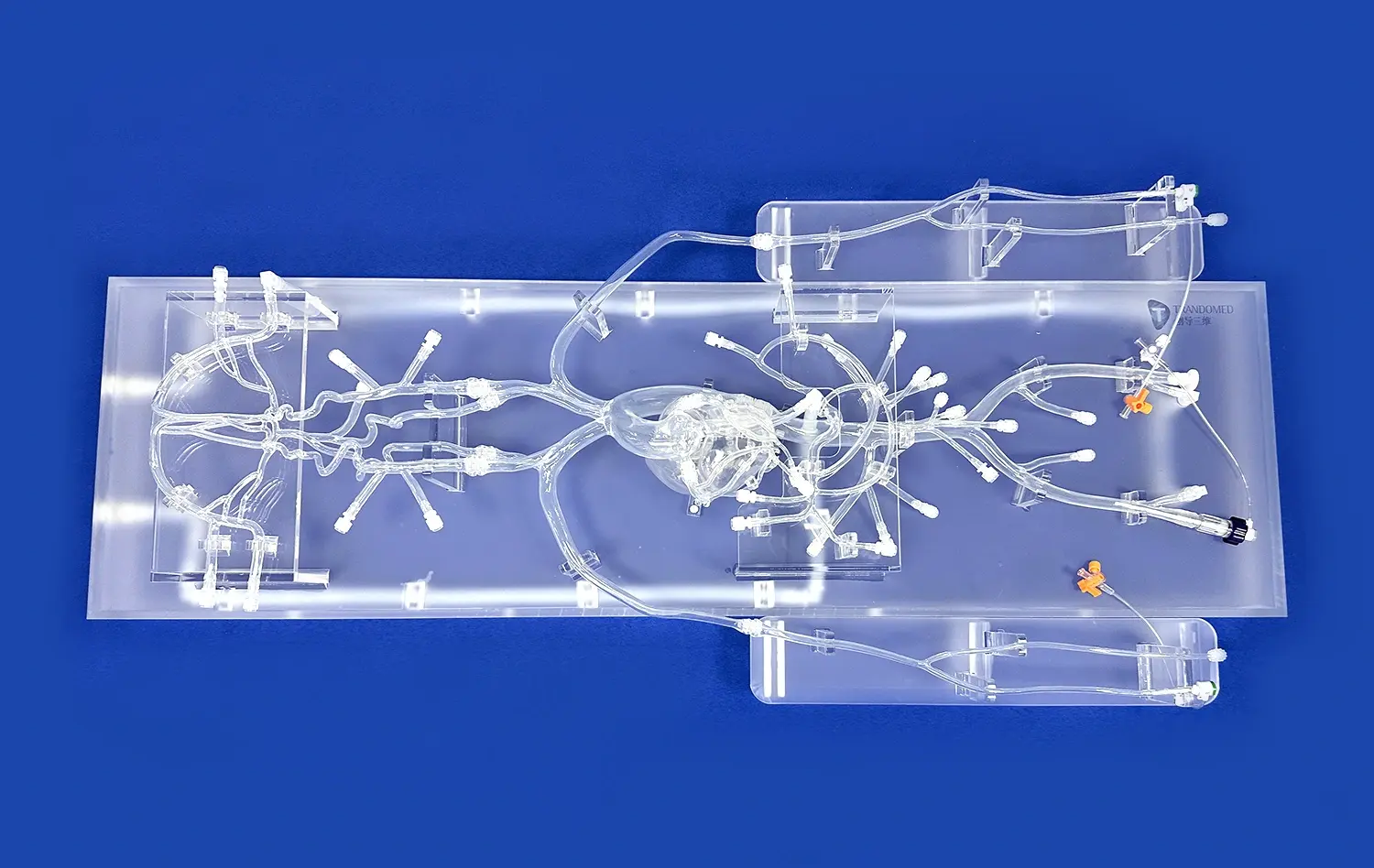
Reproducing the body in a way that is true to life is the basis of successful ASD training. Good simulation models show the whole path of an intervention, from entry points in the femur to the atrial septum itself, going through venous structures. When students work with models made of medical-grade silicone (usually Shore 40A), the tissues react in a way that is similar to how a real patient's body would. This feedback through touch is very helpful when learning how to move tubes through difficult angles or place closure devices inside holes of different sizes. The part of the atrial septum that has the ASD lesion becomes a focus point where skills can be practiced over and over again until muscle memory forms.
In addition to basic anatomy, more complex models include a number of birth defects. Different types of patent foramen ovale (PFO), ventricular septal defects (VSD), and patent ductus arteriosus (PDA) can all be trained on the same system. Because it is so flexible, schools can offer full courses without having to keep different tools for each type of condition. This flexibility is especially helpful for medical schools, where students learn about a wide range of illnesses during a single training lesson.
Material Science Enhances Realism
Silicone-based materials are very durable and still have the tissue-like qualities that are needed for procedural training. The Shore 40A hardness specification gives the right amount of resistance during catheter insertion and device deployment. This keeps things from being too easy, which would not prepare students well for clinical practice. This material doesn't break down after hundreds of practice sessions, so modeling centers that run a lot of training programs can save money by using it.
Manufacturers can now change the qualities of materials based on certain body parts. Vascular walls and heart chambers may have different densities, which is a real physiological difference. This level of attention to detail makes sure that trainees learn a lot about how tissues interact throughout the whole interventional route.
Integration With Real Medical Devices
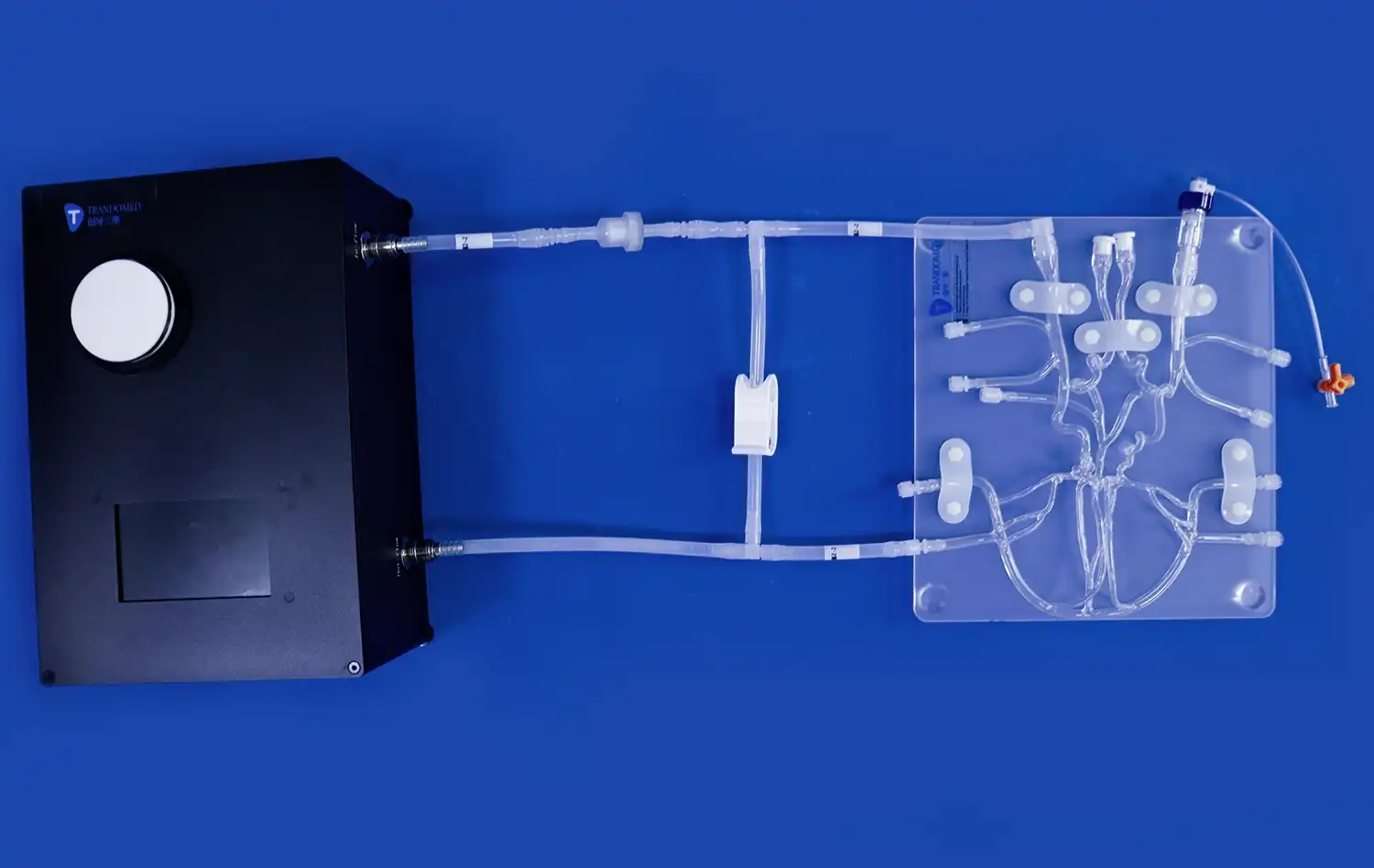
For training to be real, it needs to work with real clinical tools. Standard catheter sizes, guidewires, and ASD closure devices used in operating rooms around the world can be used with good computer congenital heart disease intervention training models. This compatibility gets rid of the fake learning setting that generic simulators make. Cardiologists can easily go from training to doing procedures when they practice with the same tools they'll use during operations.
Manufacturers of devices can also use these models to help them make and test new products. Instead of using expensive animal models or starting human trials too soon, engineers can use anatomically accurate simulators to make sure that new ASD closure systems work and find any problems that might happen before putting them on the market.
Limitations of Traditional ASD Training vs. Modern Intervention Models
The change from traditional teaching methods to simulation-based education is due to both the need to protect patients and the progress in technology.
Patient Exposure Constraints
In traditional cardiology training, junior doctors watched processes and then gradually took on more responsibility while still being supervised. Even though this method gave real-world knowledge, it naturally limited the chances to practice. During residency, each trainee might only be involved in a few ASD cases because these treatments aren't done as often as other heart procedures. Because they didn't get enough experience, practitioners often went into independent practice without enough faith in their procedures.
There are also risks that come with real patient cases that make it harder to learn. Trainees can't try out different methods or purposely make things more difficult in order to practice rescue skills. Because it is the right thing to do to put patient safety first, hands-on teaching during real procedures has to be limited.
Standardization Challenges
Because patients' bodies are very different, it's hard to make sure that all of them have the same training situations. One trainee might work on simple ASD cases with perfect anatomy, while another might work on difficult cases with defects in strange places or in structures nearby. This variety is good for schooling as a whole, but it leaves gaps in the development of basic skills.
These differences are fixed in modern simulation systems by giving standardized initial training. Before moving on to variations that reflect clinical variety, all trainees learn the basics on models with typical anatomy. This structured progression makes sure that all of the skills are developed, which is something that more traditional ways can't do.
Cost and Resource Implications
Using the operating room costs a lot of money for the hospital. Using these facilities for training puts a strain on the budget, especially when processes take longer than usual because of the trainees' presence. Simulation labs are another way to train that doesn't cost anything and lets you practice as much as you want. Trainees can practice procedures over and over until they are good at them without using up valuable clinical resources or being limited by time limits.
Researchers who compared traditional training to training based on simulations found that the latter led to measurable changes in the efficiency and rate of complications of procedures. Studies in major cardiology journals show that practitioners trained mostly through simulation methods have shorter process times and higher accuracy when deploying devices compared to those trained mostly through traditional apprenticeship models.
Selecting the Optimal Congenital Heart Disease Intervention Training Model
Before making a purchase choice, you need to carefully consider more than just the initial cost of the item. Long-term value comes from a simulation platform that is durable, flexible, and in line with the training goals of the organization.
Assessing Realism and Fidelity
High-fidelity congenital heart disease intervention training models are worth the money because they help students learn more effectively. When procurement teams are looking at their choices, they should look at the anatomical details, the properties of the materials, and how well they work with other medical devices. With models that correctly show vessel tortuosity, cardiac chamber dimensions, and defect characteristics, students can learn skills that can be used right away in real-life medical situations.
Before making big purchases, ask to see some demonstration models. Let the cardiac staff test the models with real catheters and closure devices. Their feedback on the realism of touch and the accuracy of the process should be used to make selection choices. Models like the XXS003 from specialized makers include the femoral vein, the iliac vein, the inferior vena cava (IVC), and both atrial structures on both sides, along with ASD lesions that can be changed. These models show the whole anatomy needed for full interventional training.
Customization Capabilities
Training needs change from institution to institution based on the types of patients they see, the number of procedures they do, and their educational goals. Models that can be customized without charging extra for design work are the best deals. You can make sure that the ASD is in line with your specific training program by specifying its location, size, and any surrounding anatomical differences.
Modern manufacturers can work with data files in CT, CAD, STL, STP, and STEP forms, which lets real imaging studies be used to make models that are unique to each patient. This feature is especially useful for planning surgeries ahead of time, as it lets medical teams practice difficult cases on models of real patients' bodies before they go into the operating room.
Evaluating Manufacturer Support
Supplier ties go beyond just delivering goods. Manufacturers of good products offer full technical help, training materials, and quick replacement parts. When looking at possible providers, you should ask about their experience with medical simulation, their ability to make things, and how quickly they respond to customer service requests.
Well-known companies that have been using medical 3D printing technology for decades can help with both unique projects and fixing problems. When compared to distributors who use third-party manufacturers, companies that have their own production sites usually have faster turn-around times (often 7–10 days). This speed is very important when fixing broken parts or quickly expanding training programs.
Total Cost Analysis
Effective procurement decisions balance upfront investment against long-term operational costs and training benefits. Calculate the total cost of ownership including:
- Initial model acquisition
- Replacement components for high-wear areas
- Storage and maintenance requirements
- Staff time for setup and supervision
- Training effectiveness gains translating to reduced clinical complications
Quality congenital heart disease intervention training models justify higher initial costs through durability, reduced replacement frequency, and superior learning outcomes that improve institutional reputation and patient safety metrics. Cheap alternatives that require frequent replacement or provide inadequate realism ultimately cost more while delivering inferior training results.
Implementing Training Models to Enhance ASD Intervention Skills
Getting good tools for simulations is only the beginning. Structured curricula that are used for effective execution maximize return on investment and speed up competency development.
Curriculum Development
Make teaching modules that build skills in a step-by-step way. During foundational lessons, the focus should be on teaching patients how to move a catheter through veins without rushing. As trainers show they can do the job well, add challenges like vessel tortuosity or strange anatomical variations.
Intermediate courses focus on ASD size, device choice, and deployment methods. Trainees should work with a range of gadget sizes and types to get a feel for how different systems work during placement. This exposure makes people more confident in their choices when choosing a gadget based on the characteristics of a defect.
Complication management examples are part of advanced training. Set up difficult situations on purpose, like device embolization, incorrect placement, or residual shunts, so that trainees have to figure out what's wrong and fix it. These high-stress exercises help students learn how to think critically and adapt to different situations, which are important skills for practicing on their own.
Assessment and Metrics
Objective performance measurement proves that training works and shows where more attention is needed. Set up key success indicators, such as the time it takes to finish a procedure, the amount of simulated fluoroscopy used, the accuracy of device deployment, and the speed at which complications are recognized. Track the growth of each trainee over several sessions to keep track of skill acquisition curves.
Video recording makes debriefing meetings better. When teachers watch recorded procedures, they can give specific feedback on how to handle catheters, how to make decisions, and how to improve technique. Trainees can improve faster by making specific changes based on a visual study of their performance.
Integration With Clinical Rotations
Instead of replacing actual exposure, simulation training should be used along with it. Set up training programs so that trainees can learn basic skills in simulation labs before they do real processes. This training gives them the skills to make a real difference in clinical cases instead of just watching.
Set up simulation lessons right before clinical rotations to help students remember what they've learned and figure out which skills they need more practice with. After a rotation, trainees can practice skills they saw but weren't able to use in supervised cases. This helps them remember what they've learned by putting it right away into practice.
Procurement and Investment Insights for B2B Clients
Healthcare institutions, medical device companies, and training centers all buy simulation equipment in different ways, so they need different methods for getting it.
Hospital and Training Center Considerations
Medical schools and clinical skills centers put a lot of emphasis on models that support varied curricula that cover a wide range of heart conditions. Multi-lesion platforms with customizable flaws give teachers the most freedom with their lessons while staying within their budgets. When schools look at potential suppliers, they should check the quality control measures that make sure the products meet uniform standards and follow all the rules.
When schools have tight academic schedules, shipping dependability is very important. When a supplier offers more than one foreign carrier, like FedEx, DHL, EMS, UPS, and TNT, it gives you more options for shipping, whether you need to get something quickly or save money. Lead times of 7 to 10 days allow for flexible program development without having to plan for a long time.
Medical Device Manufacturer Applications
Companies that are making ASD closure devices, catheters, or diagnostic tools need computer models for more than just training. Anatomically correct platforms that work with prototype systems are helpful for testing products, making sure designs work, and showing off products to potential buyers.
Manufacturers should look for providers that can make a lot of changes and accept engineering file formats. Product development cycles can go more quickly when models can be made quickly that match specific anatomical situations. Custom defect shapes, locations, and surrounding structures help engineers figure out how devices work with a wide range of body structures they'll see in patients.
Distributor and OEM Partnerships
When medical device distributors are looking for congenital heart disease intervention training models for their customers' education programs, they should focus on suppliers who offer white-label options and bulk discounts. Manufacturers who have been around for a while and have a wide range of products can often work with private labeling agreements that support brand identity while taking advantage of their specialized manufacturing skills.
OEM partnerships let companies get access to cutting-edge modeling technology without having to spend money on their own research and development. Because of these partnerships, distributors can offer full solutions, including both devices and training tools. This helps them stand out in the market and give customers more value than just buying products.
Conclusion
Advanced simulation platforms have completely changed ASD intervention training by creating risk-free spaces where professionals can practice important skills over and over again. Anatomical accuracy, realistic materials, and device compatibility all work together to make sure that training leads straight to clinical success. When institutions buy high-quality models from seasoned makers that offer customization options and quick support, they set the stage for better patient outcomes and professional growth. More and more proof supports simulation-based training, which means that these tools are now necessary parts of modern cardiology education and not just extras that can be added to traditional methods.
FAQ
What advantages do simulation models provide compared to traditional ASD training?
Simulation models eliminate patient risk while providing unlimited practice opportunities. Trainees can repeat procedures until achieving mastery, experiment with different techniques, and deliberately practice complication management—all impossible during actual patient cases. Standardized anatomy ensures consistent baseline training across all learners, while customizable variations introduce clinical diversity systematically. Cost savings from reduced operating room time and improved procedural efficiency typically offset equipment investment within the initial year of implementation.
How do these training tools improve patient outcomes?
Practitioners who train extensively on realistic models demonstrate measurably better performance during actual procedures. Studies document reduced fluoroscopy time, faster procedure completion, fewer device deployment complications, and enhanced complication recognition among simulation-trained cardiologists. This improved competency directly translates to better patient outcomes through reduced procedural risks, shorter anesthesia exposure, and higher success rates.
Are these models compatible with all catheter systems?
Quality simulation platforms accommodate standard catheter sizes, guidewires, and ASD closure devices used internationally. When evaluating specific models, verify compatibility with your institution's preferred equipment brands. Reputable manufacturers provide detailed specifications regarding device compatibility and can customize models to accommodate particular systems if standard configurations don't meet your requirements.
Partner With Trandomed for Advanced ASD Training Solutions
Trandomed stands as a pioneering congenital heart disease intervention training model manufacturer with over 20 years of specialized expertise in medical 3D printing technology. Our XXS003 model delivers unmatched anatomical fidelity through medical-grade silicone construction, complete femoral-to-atrial pathway replication, and customizable defect configurations tailored to your specific training needs. We eliminate design fees for customization projects and provide rapid 7-10 day production timelines supporting urgent program launches. Our comprehensive technical support ensures you maximize training effectiveness from day one. Contact jackson.chen@trandomed.com to discuss your institutional requirements and discover how our simulation platforms can elevate your cardiology training program to new standards of excellence.
References
Marshall, A. C., & Lock, J. E. (2019). "Structural and Electrophysiological Disorders of the Heart." In Moss and Adams' Heart Disease in Infants, Children, and Adolescents: Including the Fetus and Young Adult, 9th Edition. Philadelphia: Wolters Kluwer.
Baumgartner, H., De Backer, J., Babu-Narayan, S. V., et al. (2020). "2020 ESC Guidelines for the Management of Adult Congenital Heart Disease." European Heart Journal, 42(6), 563-645.
Feins, E. N., Emani, S. M., & Pigula, F. A. (2021). "Simulation-Based Training in Congenital Cardiac Surgery: A Paradigm Shift in Educational Methodology." Seminars in Thoracic and Cardiovascular Surgery: Pediatric Cardiac Surgery Annual, 24, 45-52.
Ender, J., Koncar,-Zeh, J., Mukherjee, C., et al. (2018). "Value of Augmented Reality-Enhanced Transesophageal Echocardiography (TEE) for Determining Optimal Annuloplasty Ring Size." Annals of Thoracic Surgery, 106(5), 1445-1452.
Biglino, G., Capelli, C., Wray, J., et al. (2017). "3D-Manufactured Patient-Specific Models of Congenital Heart Defects for Communication in Clinical Practice: Feasibility and Acceptability." BMJ Open, 7(6), e015205.
Anderson, R. H., Baker, E. J., Penny, D. J., et al. (2020). "Paediatric Cardiology, 4th Edition: Expert Consult - Online and Print." Philadelphia: Churchill Livingstone Elsevier.
_1734504221178.webp)