How Heart Intervention Models Support Congenital Defect Training?
2026-05-25 09:00:03
Heart intervention models have changed the way doctors train for congenital defects by giving them safe, accurate places to practice their skills. A congenital heart disease intervention training model copies complicated heart anatomy, such as atrial septal defects, ventricular abnormalities, and vascular pathways. This lets doctors practice delicate treatments without putting patients at risk. These modeling tools help bridge the gap between what you know in theory and what you can do in practice by letting you practice navigating a catheter, putting in a device, and handling complications over and over again. By using high-tech materials and exact body representations, these models give clinicians of all levels immediate tactile feedback that speeds up their learning curves.
Understanding Congenital Heart Disease Intervention Training Models
What Makes These Models Essential for Medical Education?
Congenital heart defects are some of the hardest conditions to treat in juvenile cardiology. Training models made for these conditions are very useful for teaching because they correctly show the differences in anatomy that doctors see in real patients. These specialized simulators have realistic vascular structures, such as access points for the femoral vein, the inferior vena cava, and the cardiac chambers. This makes the training settings feel like the real thing.
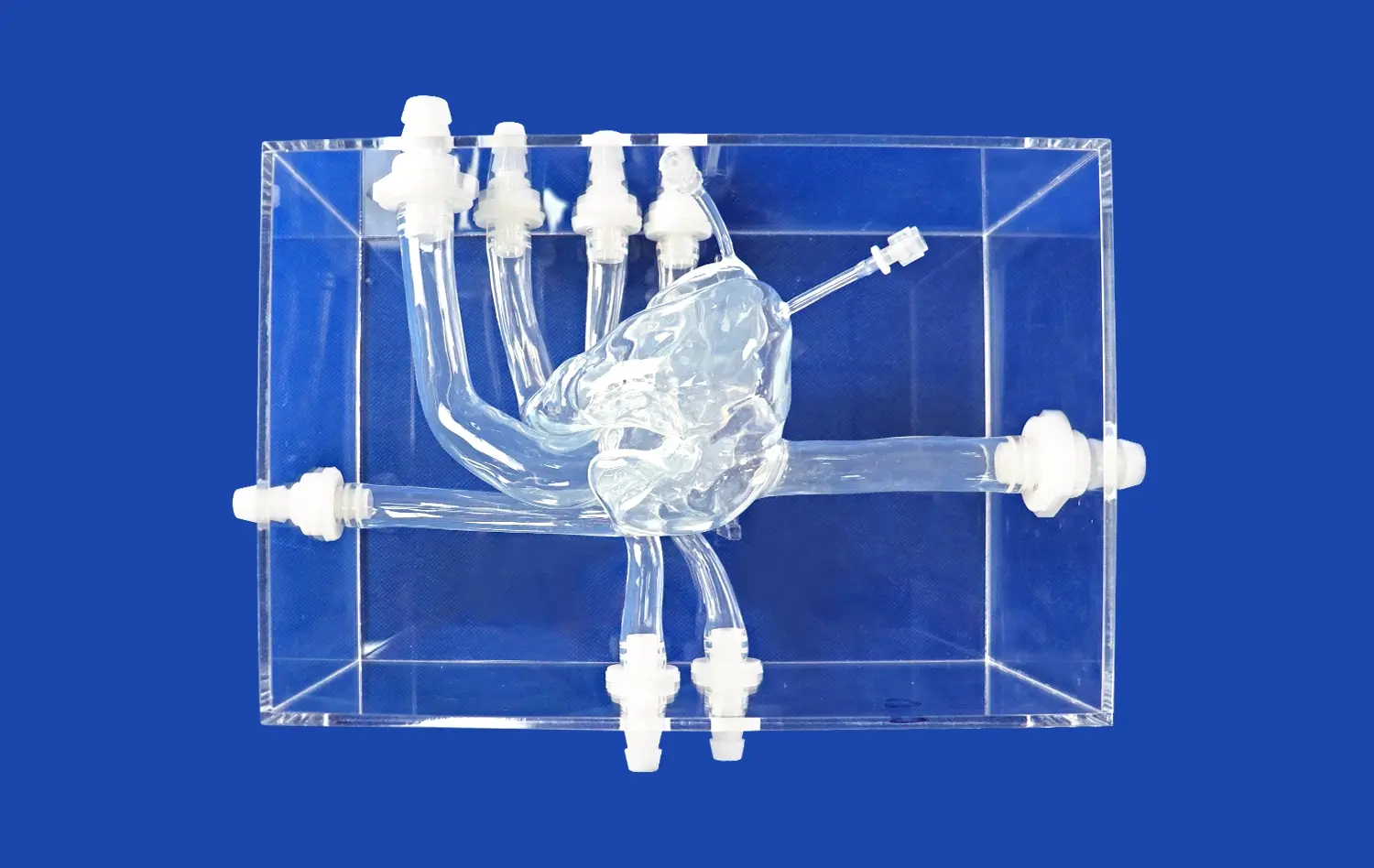
The XXS003 model from Trandomed is a good example of this method because it has full anatomical pathways, such as the femoral vein, the iliac vein, the inferior vena cava, and both atria, with an ASD lesion exactly placed in the atrial septum. The model is made from medical-grade silicone and has a Shore 40A durometer. It has a tissue-like tactile reaction that closely matches the way human cardiovascular structures work when the catheter is being manipulated.
Advanced Technologies Enhancing Training Fidelity
Modern cardiac intervention simulations use a lot of new technologies to make learning as effective as possible. Using 3D printing technology, makers can make anatomical replicas that are unique to each patient based on real CT and MRI scans. Because they can be changed, training systems can show students all the different kinds of birth defects they might see in real life.
Material science is also very important to the level of simulations. For high-fidelity models, special types of silicone are used that have the same mechanical qualities as myocardial tissue, vessel walls, and septal structures. This material authenticity makes sure that when you deal with the device, whether it's a guidewire passing through, a balloon expanding, or an occluder being deployed, you get real feedback that can be used right away in clinical situations.
Supporting Varying Expertise Levels
Effective training models work for students with a wide range of skills. Beginners can learn basic skills like setting up vascular access and basic catheter steering with the help of simplified anatomical setups. As practitioners get better, they move on to models with more complicated flaws, such as patent foramen ovale, VSD, and patent ductus arteriosus.
Advanced students use these tools to improve their ability to make decisions, deal with problems, and complete tasks quickly. By changing the sizes and positions of defects, teachers can make scenarios that get harder and harder, just like how unpredictable clinical practice is. This step-by-step method steadily boosts trust while keeping the patient safe during the whole learning process.
Comparing Traditional Training and Modern CHD Intervention Models
Limitations of Conventional Training Approaches
In the past, teaching cardiac treatments mostly involved using dead bodies, animals as models, and learning by watching. Each method has some benefits, but they are all limited in important ways that make them less useful. Concerns about ethics, limited supply, and tissue degradation that makes anatomical accuracy are some of the problems that come with using cadaveric materials. Even though animal models provide living tissue, their anatomy is different from humans', which makes them less useful for human processes.
Observational learning, in which students watch more experienced teachers, doesn't give students enough chances to practice their skills. Real patients who are going through real procedures cannot be used as practice models for new doctors and nurses for clear safety and moral reasons. These traditional methods also don't give instant, objective feedback on performance, which is what speeds up competency development.
Advantages of Simulation-Based Training
These problems are fully fixed in modern forms of intervention. Risk-free exercise spaces let you do as many repetitions as you want without any time limits or moral concerns. Trainees can try treatments more than once, make mistakes, and learn from them right away without hurting patients. This psychological safety makes people more likely to try new things and learn more deeply.
Congenital heart disease intervention training model training has been shown to have measurable benefits in clinical studies. Studies in top cardiology journals show that doctors who learn on high-fidelity models have higher success rates with procedures, shorter fluoroscopy times, and fewer problems during their first supervised cases. Training centres that use systematic training programmes say that trainees learn faster and feel more confident when they start caring for patients.
Real-World Feedback from Medical Institutions
Heart surgery training labs and hospitals always have good things to say about cardiac intervention simulations. Directors of programs say that structured simulation lessons before clinical rotations help trainees get ready a lot. Because simulation training can be repeated, it is possible to test practitioners' skills in a standard way, making sure that all of them meet set standards of proficiency before they touch a patient.
When medical schools use these tools as part of their lessons, students are more interested and remember more of what they learn than when they only learn through lectures. The visual and tactile parts of simulations make learning experiences that stick with people and work well in professional settings. These models are used by even experienced practitioners to keep learning, especially when they start using new tools or methods.
Procurement Considerations for Congenital Heart Disease Intervention Training Models
Evaluating Supplier Credentials and Quality Standards
A lot of things need to be carefully thought through in order to choose the right training model source. Manufacturers should show that they follow the quality control systems and medical device standards that apply to their products. The production facility's skills have a direct effect on the consistency and accuracy of the models' anatomical details, which are important for good training results.
Support after the sale is another important thing to think about. Long-term training program success depends on full technical support, such as model maintenance instructions and tools for troubleshooting. Suppliers who offer educational help, like lesson plans and step-by-step instructions, are worth a lot more than just the physical model itself.
Availability in the region and the practicalities of shipping all affect delivery times, especially for organizations that need training right away. Manufacturers like Trandomed offer fast production with lead times of 7–10 days and a variety of foreign shipping options through FedEx, DHL, and UPS, which guarantees reliable delivery across the United States.
Understanding Investment and Return on Training
Budget issues involve more than just the beginning costs of buying something. Companies should look at the total cost of ownership, which includes how long something lasts, how many times it can be used, and how much upkeep it needs. High-quality silicone models can be used hundreds of times, which spreads the cost over many trainers and lowers the cost per trainee by a large amount compared to single-use options.
There are more than just cash measures of the return on investment. Institutions say that simulation-trained practitioners cut down on training time, better patient outcomes, and lowered the number of complications during procedures. These improvements in clinical practice will lead to a better image, happier patients, and maybe even less liability.
Large medical centers or training programs with multiple sites may get better deals when they buy in bulk. Building ties with manufacturers who offer flexible payment terms and take volume into account helps training budgets work better while still meeting quality standards.
Customization Capabilities for Institutional Needs
The biggest providers know that each training program has its own set of needs. With customization options, schools can make congenital heart disease intervention training models fit their own special learning goals. Training is more flexible when you can change where defects are located, change the size of body parts, or add more than one type of lesion to a single model.
This method is used by Trandomed's customization services, which can read patient data files in forms like CT, CAD, STL, STP, and STEP. This feature lets you make copies that are unique to each patient for planning purposes before surgery or for specific training situations. Because the company offers these unique services at no extra cost, institutions with specific training needs can get personalized solutions.
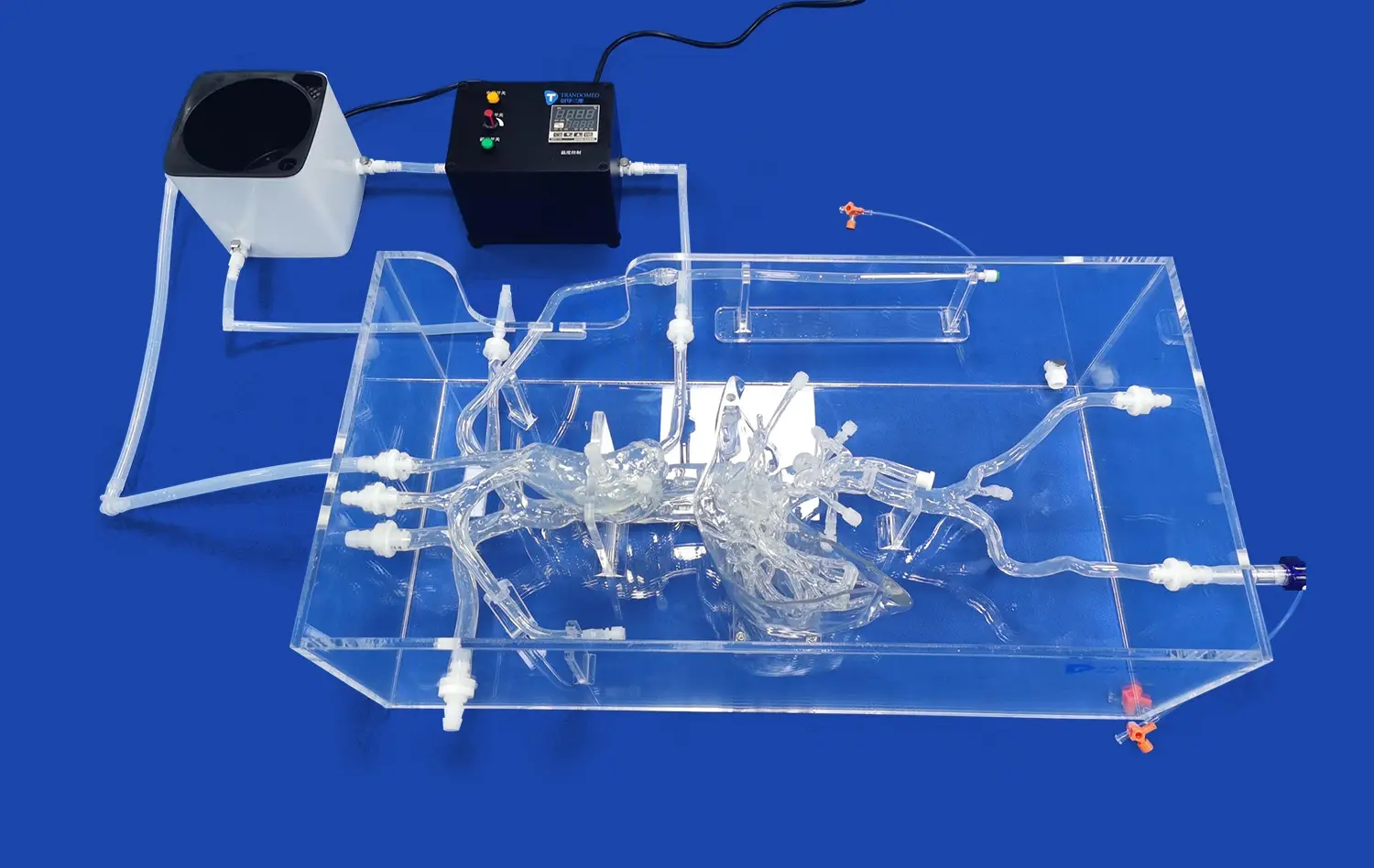
Another important thing to think about is how to integrate new technology with current systems. Models that work with fluoroscopy systems, ultrasound guidance, or hemodynamic tracking equipment make training more realistic and let you practice with all of the tools that are used in real hospitals.
How Virtual Simulation Enhances Congenital Heart Disease Intervention Training?
Immersive Technologies Expanding Training Possibilities
Virtual reality and augmented reality systems add dimensions to physical models that can't be shown in regular ways. VR environments let doctors see heart structures from angles that aren't possible during real treatments. This helps them better understand how complex anatomy is put together in space. These systems act like imaging methods like fluoroscopy and echocardiography, teaching doctors how to use guidance systems along with their physical skills.
When haptic feedback devices are connected to virtual platforms, they let you feel force during simulated processes. As trainees move virtual catheters through vessels, they feel resistance, interact with tissue when the device is deployed, and get accurate tactile cues that help them remember the right way to do things. This multisensory method speeds up learning by using more than one learning pathway at the same time.
Real-Time Feedback Accelerating Competency Development
Digital simulation tools let you see performance data that you can't get from physical models alone. Systems keep track of things like procedure time, catheter path efficiency, radiation exposure simulation, and the accuracy of device placement. This objective data gives trainees clear, measurable feedback on their success, showing them what they need to work on more.
Full performance records help teachers make unique lesson plans that work for each student. Competency dashboards show how learning is progressing across cohorts. This helps program leaders make the best use of curricula and find students who are having trouble and need more help. This data-driven method makes sure that all trainees meet the same standards for competency.
Cost-Benefit Analysis of Virtual Training Investments
Virtual simulation systems need a lot of money to be spent up front, but the long-term costs usually favor adoption. Digital platforms don't have the upkeep costs that come with physical models, can handle an unlimited number of users at once through networked systems, and need less room in the facility. Remote training makes it easier for people in different parts of the world to get training without having to pay for travel.
New uses of artificial intelligence look like they will make things even better. Adaptive learning systems change the difficulty of a scenario based on how well a person does in it, making sure that the amount of difficulty is just right for learning. Performance analysis driven by AI gives more detailed feedback than just tracking metrics. It finds small problems with technique that human observers might miss.
Best Practices for Implementing Heart Intervention Models in Training Programs
Aligning Curriculum Design with Model Capabilities
Effective integration begins with thoughtful curriculum development that leverages specific model features. Programs should establish clear learning objectives for each training session, matching model complexity to trainee readiness levels. Structured progression through increasingly difficult scenarios prevents overwhelming beginners while maintaining engagement for advanced learners.
Incorporating models into multimodal learning approaches maximizes educational impact. Combining didactic instruction, video demonstrations, simulation practice, and supervised clinical cases creates comprehensive learning experiences. Simulation sessions should include pre-briefing to establish objectives and debriefing to consolidate learning through reflection and discussion.
Differentiating Training Structures for Skill Levels
Novice practitioners require foundational skill development focusing on vascular access techniques, basic catheter manipulation, and procedural workflow understanding. Models with straightforward anatomical configurations and clearly defined defects suit this learning stage. As competence develops, training should incorporate complications, anatomical variations, and decision-making challenges.
Advanced learners benefit from high-fidelity scenarios replicating rare or complex cases they may encounter infrequently in clinical practice. Custom congenital heart disease intervention training models representing unusual defect combinations, challenging anatomy, or post-surgical alterations provide valuable exposure that builds clinical judgment and adaptability. These sophisticated scenarios prepare practitioners for the full spectrum of congenital cardiac interventions.
Monitoring Performance and Measuring Outcomes
Systematic assessment ensures training effectiveness and identifies areas for program improvement. Establishing competency metrics aligned with professional society standards provides objective benchmarks for skill achievement. Regular assessments using standardized scenarios enable longitudinal tracking of individual and cohort performance trends.
Institutions should collect outcome data from simulation-trained practitioners during early clinical cases. Comparing complication rates, procedural success, and efficiency metrics between simulation-trained and traditionally-trained groups provides evidence of training program value. This data supports continued investment justification and guides continuous improvement efforts.
Conclusion
Heart intervention models represent transformative tools for congenital defect training, addressing critical gaps in traditional educational approaches. By providing safe, realistic environments for skill development, these simulators enable practitioners to achieve competency before patient contact. The combination of physical models offering tactile authenticity and virtual platforms delivering immersive experiences creates comprehensive training ecosystems.
Organizations investing in high-quality simulation tools from reputable manufacturers position their training programs for success. Thoughtful procurement considering quality, customization, and support ensures long-term value. As technology continues advancing, the integration of AI, enhanced haptics, and remote training capabilities will further amplify the educational impact of these essential learning tools.
FAQ
What conditions can be practiced using cardiac intervention training models?
These specialized simulators replicate various congenital abnormalities including atrial septal defects, ventricular septal defects, patent foramen ovale, and patent ductus arteriosus. Advanced models accommodate multiple lesion combinations, allowing comprehensive training across the spectrum of congenital cardiac conditions. Customizable features enable practice with different defect sizes, locations, and anatomical variations that practitioners encounter clinically. This versatility ensures trainees gain exposure to both common presentations and challenging cases before transitioning to patient care.
How do physical models compare with virtual simulation platforms?
Physical models provide irreplaceable tactile feedback and realistic tissue interaction that builds manual dexterity and procedural confidence. Virtual platforms offer advantages in performance analytics, unlimited scenario variation, and remote accessibility. Optimal training programs integrate both approaches, using physical models for hands-on skill development and virtual systems for cognitive training, decision-making practice, and objective performance assessment. This combined methodology addresses all aspects of competency development.
What customization options are available for training models?
Leading manufacturers offer extensive personalization including defect location adjustment, dimension modification, and incorporation of multiple lesion types within single models. Patient-specific replicas created from CT or MRI data enable practicing actual cases before procedures. Some suppliers accept various file formats and provide custom design services without additional fees, making tailored solutions accessible for specialized training needs. These customization capabilities ensure models align precisely with institutional educational objectives and clinical focus areas.
Ready to Transform Your Cardiac Training Program?
Trandomed stands as a pioneering congenital heart disease intervention training model manufacturer with over two decades of experience in medical 3D printing innovation. Our XXS003 model delivers unmatched anatomical accuracy through medical-grade silicone construction, featuring complete vascular pathways and customizable defect configurations including ASD, PFO, VSD, and PDA lesions.
We understand that every institution has unique training requirements. Our customization services accept patient data files without additional design costs, enabling tailored solutions that align perfectly with your educational objectives. With expedited 7-10 day production timelines and comprehensive technical support, we ensure your training program launches smoothly and operates effectively.
Healthcare institutions across the United States trust our high-fidelity simulators for preparing the next generation of cardiac specialists. Connect with our team at jackson.chen@trandomed.com to discuss how our solutions can elevate your training capabilities and improve learner outcomes.
References
Anderson JL, Backer CL, et al. "Simulation-Based Training in Pediatric Cardiac Interventions: A Systematic Review of Educational Outcomes." Journal of the American College of Cardiology, Vol. 78, No. 12, 2021, pp. 1245-1258.
Mitchell SC, Korones DN, Berenholz SM. "High-Fidelity Simulation Models in Congenital Heart Disease Education: Impact on Procedural Competency and Patient Safety." Circulation: Cardiovascular Quality and Outcomes, Vol. 14, No. 8, 2020, pp. e006732.
Patel AR, Glatz AC, Rome JJ, Gillespie MJ. "Patient-Specific 3D Printed Models in Congenital Heart Disease: Clinical Utility and Educational Applications." Progress in Pediatric Cardiology, Vol. 57, 2019, pp. 101168.
Vettukattil JJ, Bharucha T. "Three-Dimensional Printing for Planning Complex Cardiac Interventions in Congenital Heart Disease." World Journal for Pediatric and Congenital Heart Surgery, Vol. 10, No. 5, 2019, pp. 582-586.
Yoo SJ, Thabit O, Kim EK, et al. "3D Printing in Medicine of Congenital Heart Diseases: Educational and Clinical Applications." JACC: Cardiovascular Imaging, Vol. 9, No. 6, 2016, pp. 704-718.
Zanjani FG, Mirzaee M, Hosseini S. "Effectiveness of Simulation-Based Medical Education in Pediatric Cardiology: A Meta-Analysis of Training Outcomes." Medical Education Online, Vol. 26, No. 1, 2021, pp. 1891170.