Left Atrial Appendage Closure Simulator for ASD and LAAO Practice
2026-05-26 09:00:04
To get good at left atrial appendage occlusion, you need to be precise, have faith, and do a lot of hands-on training. Medical workers can practice these tricky heart procedures in a safe place with a left atrial appendage closure simulator. This bridges the gap between what they learn in school and how they use what they learn in the real world. By simulating real heart anatomy and procedural challenges, these advanced training tools help doctors get better at their skills before they treat real patients. This improves patient safety and clinical outcomes across all healthcare institutions.
Understanding Left Atrial Appendage Closure Simulators
The left atrial lobe is an important part of heart function, especially for people with atrial fibrillation who are more likely to have a stroke. According to studies published in medical journals, this small sac-like structure in the left atrium is what causes about 90% of thrombus formation in people with atrial fibrillation that doesn't involve the valves. Understanding its anatomical differences is necessary for the procedure to go well.
Anatomical Complexity and Clinical Significance
Large imaging studies that followed groups of patients have found four different shapes of LAA: chicken wing (48% of cases), cactus (30%), windsock (19%), and cauliflower (3%). Each morphology creates its own set of problems for methods used to deploy and close the device. To prepare interventionalists for the wide range of patient anatomy they will see in real life, a good simulation device must properly replicate these differences.
How Advanced Simulators Replicate Cardiac Structures?
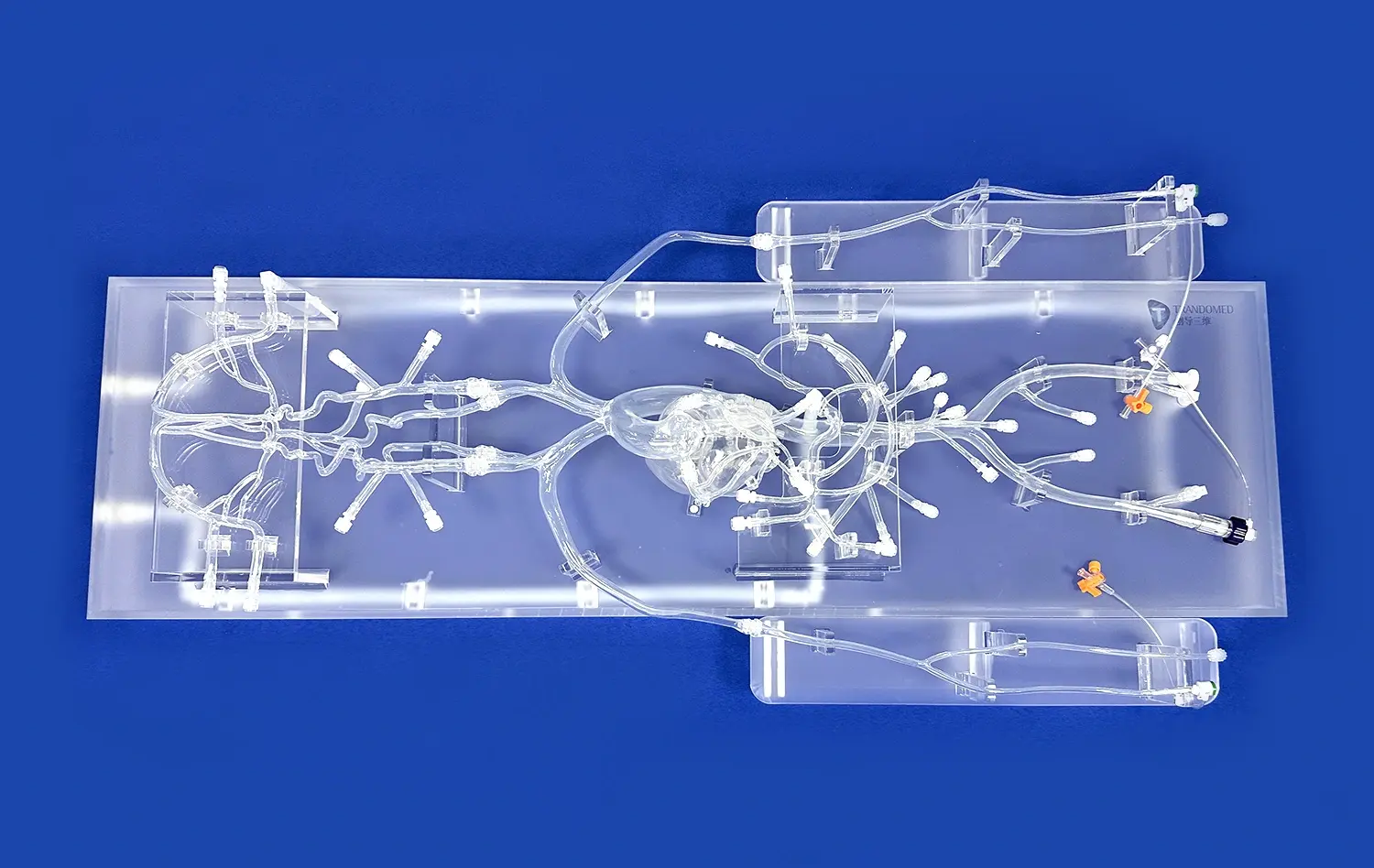
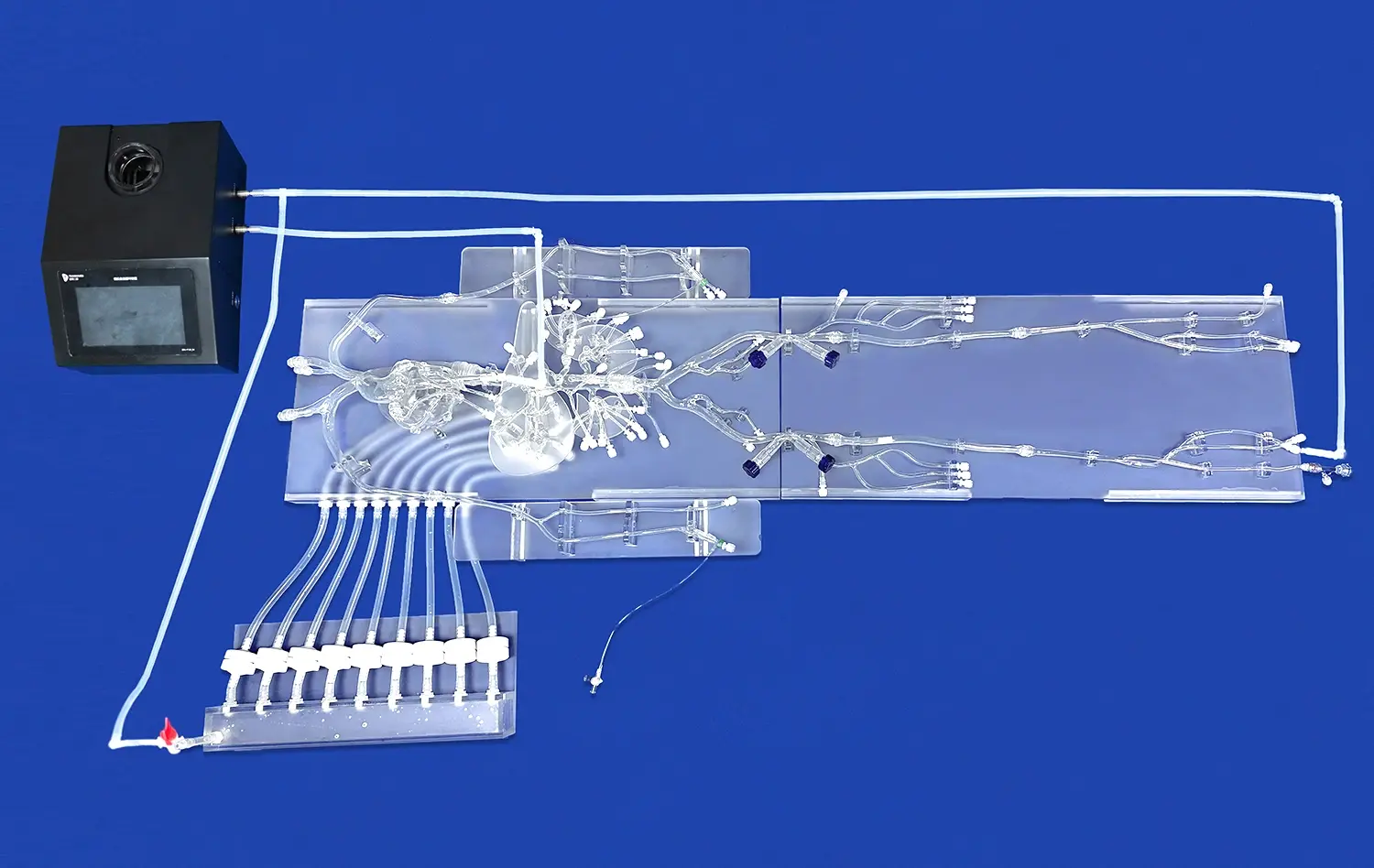
Modern cardiovascular training models have accurate anatomy that goes from access points in the femur to the heart chambers and the whole vein pathway. This all-around method is shown by the XX013D model from Trandomed, which includes the LAA and the femoral vein, iliac vein, inferior vena cava, right atrium, interatrial septum, left atrium, and pulmonary veins. This full vascular pathway lets trainees practice the whole procedure, from navigating the catheter to transseptal puncture, device placement, and final deployment.
Material Innovation in Simulation Technology
Material choice has a big impact on how realistic computer models feel when you touch them. Medical-grade silicone with a Shore hardness of 40A closely matches the qualities of human tissue, giving real haptic feedback when manipulating the catheter or putting the device in place. Because the material is always the same, professionals can build muscle memory and learn to recognize subtle tactile cues that show them how to place devices correctly or spot potential problems before they happen in real clinical settings.
Comparing Left Atrial Appendage Closure Training Methods
Medical education has changed a lot from the old ways of doing things, which mostly involved watching others, studying textbooks, and not getting much hands-on experience. Knowing the pros and cons of different training methods helps people in charge of making decisions at institutions choose the best educational investments for their programs.
Traditional Cadaver-Based Training Limitations
Cadaver labs have been important parts of medical education for a long time, but they make it hard to learn invasive cardiology. Access is limited by ethical concerns, problems with procurement, and high prices. Because cadaveric tissue isn't as flexible and sensitive as living tissue, it doesn't give full feedback when the catheter is moved. The lack of fluoroscopic guidance, blood flow simulations, or heart motion simulations makes cadaver-based practice lessons even less realistic.
Physical Simulator Advantages
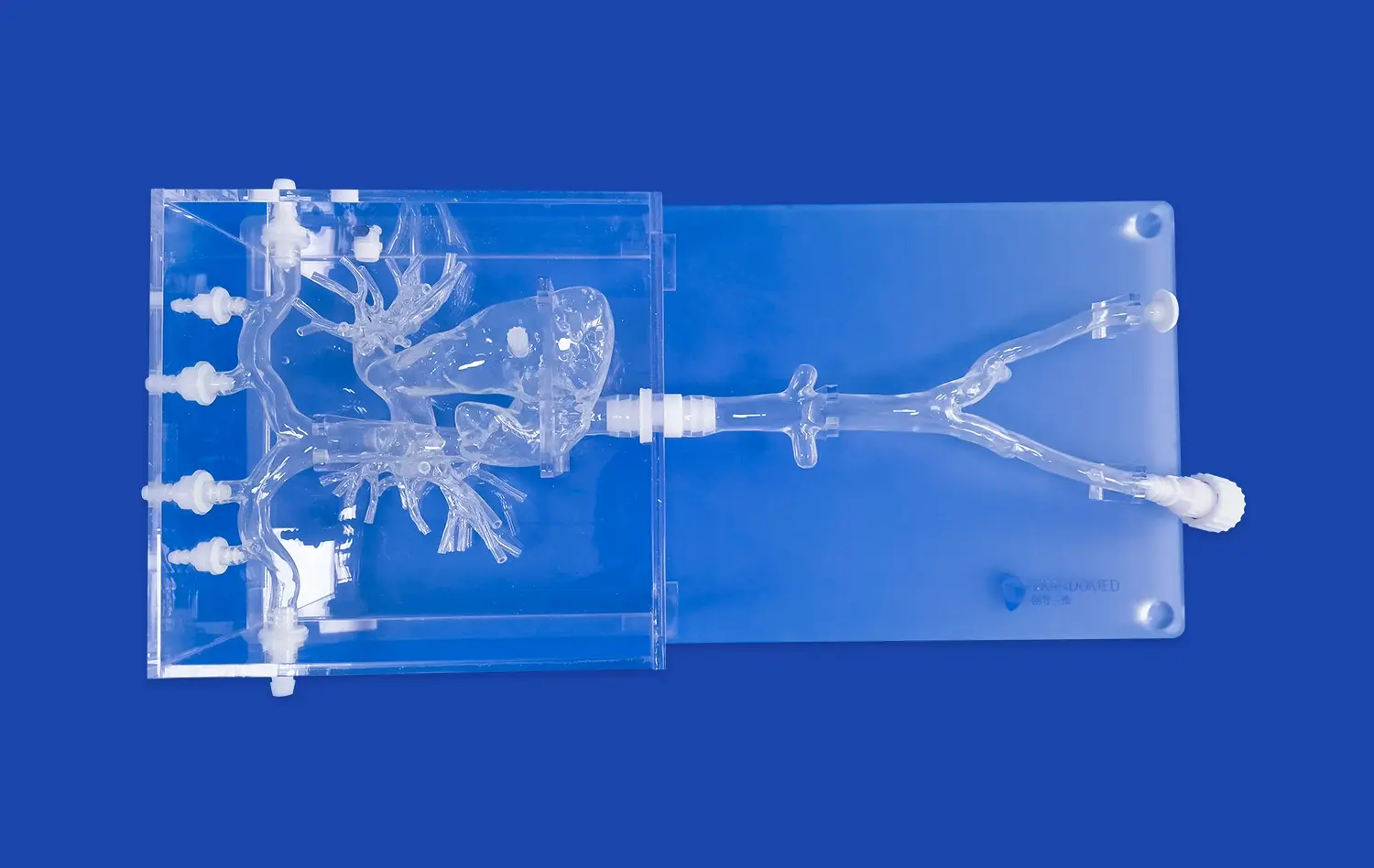
High-fidelity physical left atrial appendage closure simulators get around many of the problems with standard training while also providing unique benefits that work well with other teaching methods. These gadgets let you practice over and over again without having to worry about ethics or tissue degradation. The XX013D simulator has four different LAA shapes and three different-sized atrial septal defects. This lets you train for all possible scenarios, which would take a lot of dead bodies to do the same job.
Institutions that use physical training programs say that trainees' competency levels have gotten better. Studies in interventional cardiology journals show that doctors who were trained through simulations reach procedural milestones faster and with fewer problems in supervised clinical cases than doctors who were taught only by watching others do the procedure.
Comparing Simulator Types and Training Outcomes
Virtual reality platforms are better at adapting to different situations and keeping track of data, but physical models are better because they give you feedback that you can't get from a screen. This is especially important for catheter-based treatments. Being able to feel the resistance of tissues, understand anatomical landmarks through touch, and work with real medical gadgets all make training experiences that can be used right away in clinical settings. The best way to make training programs that cover everything right now is to use hybrid methods that combine physical models with imaging guiding systems.
Procurement Guide: How to Choose and Buy a Left Atrial Appendage Closure Simulator?
Selecting appropriate simulation equipment requires careful evaluation of institutional needs, training objectives, and technical specifications that directly impact educational effectiveness. Procurement teams benefit from structured assessment frameworks that align device capabilities with end-user requirements.
Assessing Institutional Training Requirements
Medical schools prioritize anatomical accuracy and durability to withstand repeated use by multiple trainees at varying skill levels. Hospital-based training departments focus on procedural realism that mirrors their specific patient populations and device inventory. Research institutions require customization capabilities to support experimental protocols and novel device testing. Clearly defining these priorities guides the selection process toward solutions that deliver maximum educational value.
Critical Technical Specifications
Several technical factors determine a simulator's training effectiveness and operational lifespan. Anatomical accuracy validated against medical imaging data ensures trainees develop skills directly transferable to patient care. Material durability affects long-term cost-effectiveness, particularly in high-volume training environments. Component modularity and replaceability extend device utility while controlling ongoing costs.
The XX013D simulator addresses these requirements through several engineering solutions. Its design incorporates actual patient CT and MRI data processed through reverse 3D reconstruction technology, ensuring anatomical fidelity. The inclusion of replaceable ASD components and interchangeable LAA morphologies maximizes training scenario diversity while containing costs compared to purchasing multiple dedicated models.
Customization Capabilities and Support Services
Leading simulation device manufacturers offer customization services that tailor standard products to specific institutional requirements. The ability to modify ASD dimensions, adjust anatomical landmarks, or incorporate patient-specific anatomy from provided imaging data significantly enhances training relevance. Trandomed accepts data files in multiple formats including CT, CAD, STL, STP, and STEP, enabling seamless integration of custom requirements without charging additional design fees.
Evaluating Total Cost of Ownership
Beyond initial purchase considerations, procurement professionals should evaluate shipping logistics, payment terms, and warranty coverage. The XX013D model ships via major international carriers including FedEx, DHL, EMS, UPS, and TNT with delivery timeframes of 7-10 days. Payment through bank transfer arrangements provides financial transparency and documentation necessary for institutional procurement protocols.
Verifying Simulator Effectiveness: Scientific Validation and User Experiences
Evidence-based medicine extends to educational interventions, requiring objective validation of training tool effectiveness before widespread adoption. Multiple research methodologies contribute to establishing the clinical value of simulation-based training programs.
Scientific Studies Supporting Simulation Training
Peer-reviewed publications in cardiovascular medicine journals consistently demonstrate that simulation-trained practitioners achieve superior procedural outcomes compared to traditionally trained counterparts. Randomized controlled trials measuring performance metrics such as procedure time, fluoroscopy exposure, contrast volume, and complication rates reveal statistically significant improvements among simulation-trained groups.
User Testimonials from Clinical Educators
Interventional cardiologists implementing simulation programs report accelerated learning curves and enhanced trainee confidence when transitioning to supervised clinical cases. Program directors note that simulation training allows for standardized curriculum delivery and objective competency assessment before granting independent procedural privileges. Device manufacturers conducting product demonstrations on high-fidelity left atrial appendage closure simulators receive positive feedback regarding the realistic representation of device behavior and deployment challenges.
Emerging Technologies Enhancing Simulation Value
Artificial intelligence integration promises to further elevate training effectiveness through automated performance analysis and personalized feedback. Remote training capabilities enabled by connected simulation platforms expand access to expert instruction regardless of geographic constraints. These technological advances represent substantial value for institutions seeking future-proof educational investments that adapt to evolving training methodologies and clinical standards.
Best Practices for Training with Left Atrial Appendage Closure Simulators
Maximizing educational return on simulator investments requires thoughtful integration into comprehensive training curricula rather than isolated practice sessions. Structured implementation frameworks ensure consistent skill development and measurable competency outcomes.
Structured Skill Progression Protocols
Effective simulation training follows deliberate practice principles with clearly defined learning objectives at progressive difficulty levels. Novice trainees begin with basic catheter navigation and anatomical orientation before advancing to transseptal puncture techniques. Intermediate practitioners focus on device selection, positioning, and deployment across various LAA morphologies. Advanced training incorporates complication management and rescue techniques for suboptimal deployments.
Integration with Continuous Medical Education Programs
Simulation training should complement rather than replace other educational modalities within comprehensive curricula. Combining didactic instruction, simulation practice, observation of expert practitioners, and supervised clinical experience creates robust training pathways. Incorporating simulation-based assessments into certification processes provides objective competency verification that enhances program credibility and regulatory compliance.
Maintenance and Performance Optimization
Regular inspection and maintenance protocols preserve simulator functionality and extend operational lifespan. Cleaning procedures appropriate for medical-grade silicone prevent material degradation. Tracking component replacement intervals ensures consistent training experiences. Maintaining detailed usage logs helps institutions calculate per-trainee costs and demonstrate educational investment value to administrators and accrediting bodies.
Conclusion
Advanced cardiac intervention training demands realistic, repeatable, and risk-free practice opportunities that traditional methods cannot adequately provide. High-fidelity physical simulators incorporating authentic anatomical features, diverse morphological variations, and customizable components represent essential educational infrastructure for institutions committed to training excellence. The XX013D left atrial appendage closure simulator delivers comprehensive training capabilities through evidence-based design, quality materials, and flexible customization options that address the diverse needs of medical schools, hospitals, research facilities, and training centers across the cardiovascular medicine spectrum.
FAQ
What procedures can be practiced using LAA closure simulators?
These specialized training devices support multiple cardiovascular interventions beyond basic left atrial appendage occlusion. Practitioners develop skills in femoral venous access, catheter navigation through complex vascular anatomy, transseptal puncture techniques, and pulmonary vein isolation procedures. The inclusion of multiple ASD sizes enables congenital defect repair training, while various LAA morphologies prepare interventionalists for the full spectrum of patient anatomies encountered in clinical practice.
How does simulator training compare to actual patient procedures?
High-quality simulators constructed from medical-grade materials with anatomical accuracy validated against imaging data provide remarkably realistic procedural experiences. While no training modality perfectly replicates every aspect of living tissue and clinical environments, physical simulators effectively bridge the gap between theoretical knowledge and hands-on clinical application, allowing practitioners to develop technical proficiency and procedural confidence before treating patients.
What customization options benefit research applications?
Research institutions conducting device development studies or biomechanical investigations require simulation platforms adaptable to specific experimental protocols. Custom manufacturing based on provided imaging data enables patient-specific modeling for surgical planning research. Adjustable ASD dimensions and LAA configurations support comparative effectiveness studies across anatomical variations, providing controlled experimental conditions impossible to achieve with clinical populations or cadaveric specimens.
Partner with a Trusted Left Atrial Appendage Closure Simulator Manufacturer
Trandomed stands as a pioneering left atrial appendage closure simulator supplier with over two decades of specialized expertise in medical 3D printing technology and cardiovascular training device development. Our XX013D simulator represents the culmination of extensive research incorporating real patient imaging data, proprietary manufacturing processes, and rigorous quality assurance protocols. We provide comprehensive customization services without design fees, accepting imaging data in multiple formats to create precisely tailored solutions for your institutional training objectives. Healthcare organizations, medical device companies, and research institutions benefit from our rapid production timelines, flexible payment terms, and responsive technical support throughout product lifecycles. Contact jackson.chen@trandomed.com to discuss your specific training requirements and receive detailed product information, demonstrations, and procurement guidance from our experienced team committed to advancing cardiovascular education through innovative simulation technology.
References
Di Biase L, Santangeli P, Anselmino M, et al. "Does the Left Atrial Appendage Morphology Correlate with the Risk of Stroke in Patients with Atrial Fibrillation?" Journal of the American College of Cardiology, 2012.
Holmes DR, Kar S, Price MJ, et al. "Prospective Randomized Evaluation of the Watchman Left Atrial Appendage Closure Device in Patients with Atrial Fibrillation Versus Long-Term Warfarin Therapy: The PREVAIL Trial." Journal of the American College of Cardiology, 2014.
Barsness KA, Rooney DM, Davis LM. "Collaboration in Simulation: The Development and Initial Validation of a Novel Thoracoscopic Neonatal Simulator." Journal of Pediatric Surgery, 2013.
Stefanidis D, Korndorffer JR, Heniford BT, Scott DJ. "Limited Feedback and Video Tutorials Optimize Learning and Resource Utilization During Laparoscopic Simulator Training." Surgery, 2007.
Aggarwal R, Mytton OT, Derbrew M, et al. "Training and Simulation for Patient Safety." Quality and Safety in Health Care, 2010.
Carnahan H, Dubrowski A, Rickets I. "The Role of Haptic Feedback in Simulation-Based Training." Current Opinion in Anaesthesiology, 2007.