The way pediatric cardiology is taught has changed a lot. Now, congenital heart disease intervention training models are important tools for doctors. These anatomically accurate simulators make complex heart defects like atrial septal defects, ventricular septal defects, and patent ductus arteriosus look like they really exist. This lets doctors practice delicate treatments without putting patients at risk. These training platforms close the gap between academic knowledge and clinical skill by combining realistic touch with exact procedure. They meet the urgent need for standardized, repeatable education in treating congenital heart conditions.
Understanding Congenital Heart Disease Intervention Training Models
What Makes These Training Tools Essential?
Today's pediatric cardiac education meets a major problem: congenital heart defects come in a huge range of shapes and sizes, but there are only so many chances to train with real patients. Physical simulation models fill in this gap by simulating the disease of a specific patient in a controlled setting. Synthetic simulators, unlike cadaveric specimens or animal models, let students practice as much as they want, which is important for developing muscle memory and spatial awareness for catheter-based interventions.
Anatomical Components and Structural Design
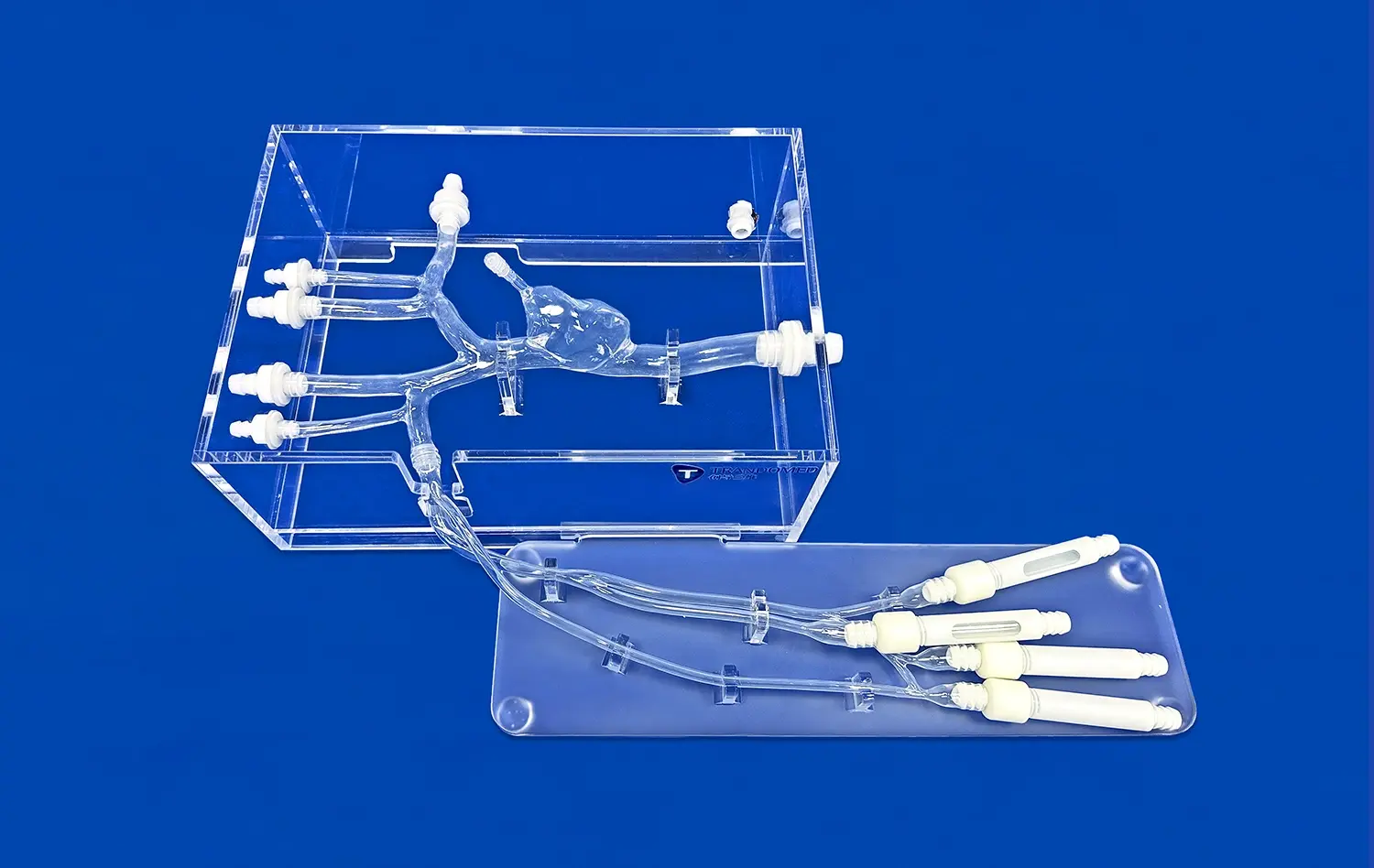
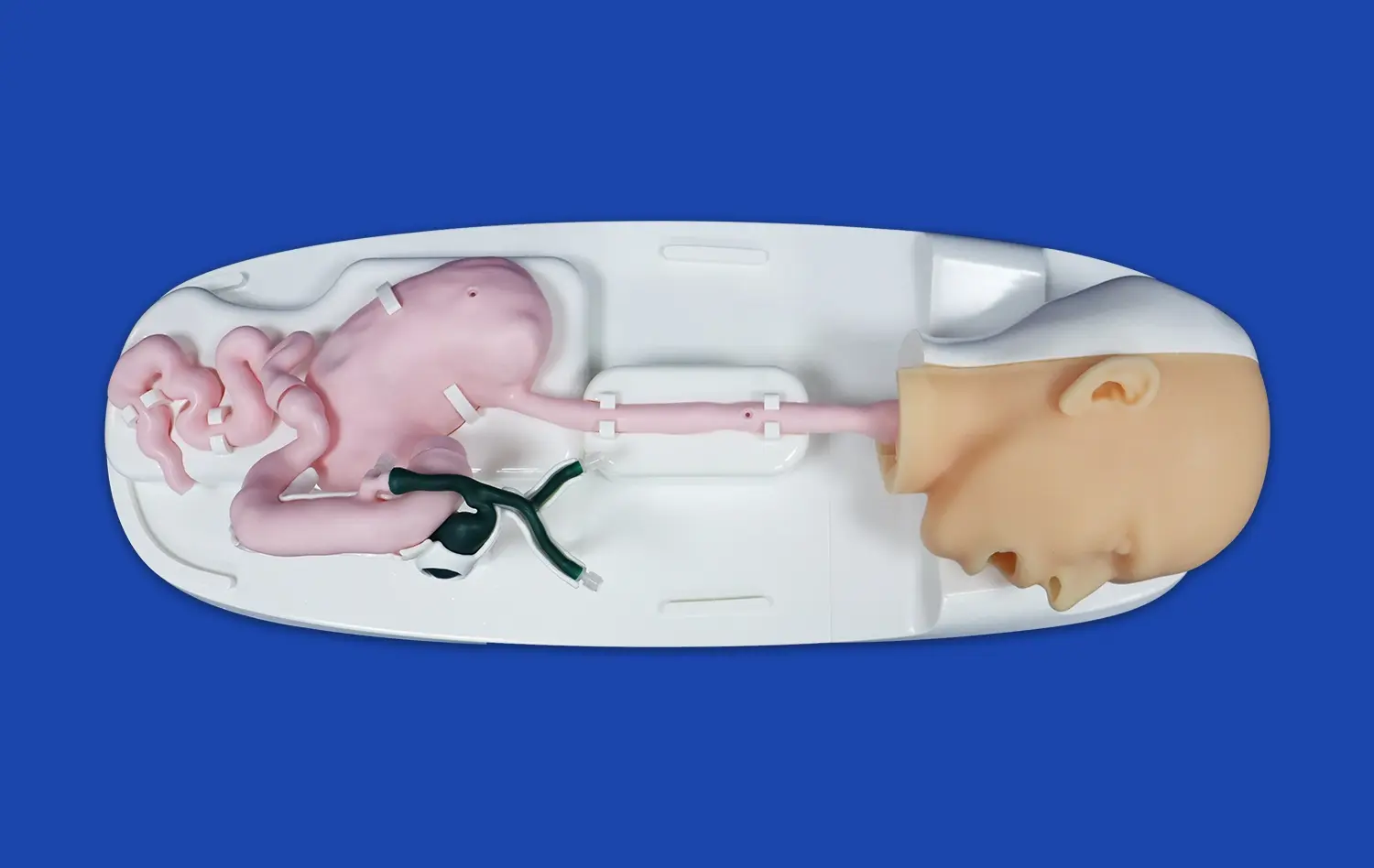
Several important vascular systems are included in high-fidelity models. During treatments, cardiologists use the femoral vein access point, the iliac vein pathway, and the inferior vena cava to plan their routes. The left and right atrial chambers are modeled with the proper sizes based on anatomy, and the atrial septum has defects that can be changed from simple secundum ASDs to more complex primum variations. This structure completeness lets trainees experience the whole process, from accessing peripherals to deploying devices.
Material Science Behind Realistic Simulation
The way training models feel has a big effect on how well skills are transferred to real life. Medical-grade silicone with a hardness of 40A Shore is like human tissue in that it doesn't give way easily when the tube is moved or the device is put in place. This choice of material makes sure that trainees learn how to use the right amount of force—too much pressure can cause puncture, while not enough force can cause the device to not be properly positioned. Because silicone is long-lasting, it can be used over and over again without losing its shape. This makes it a cost-effective choice for long-term training.
Technology Integration and Interactive Features
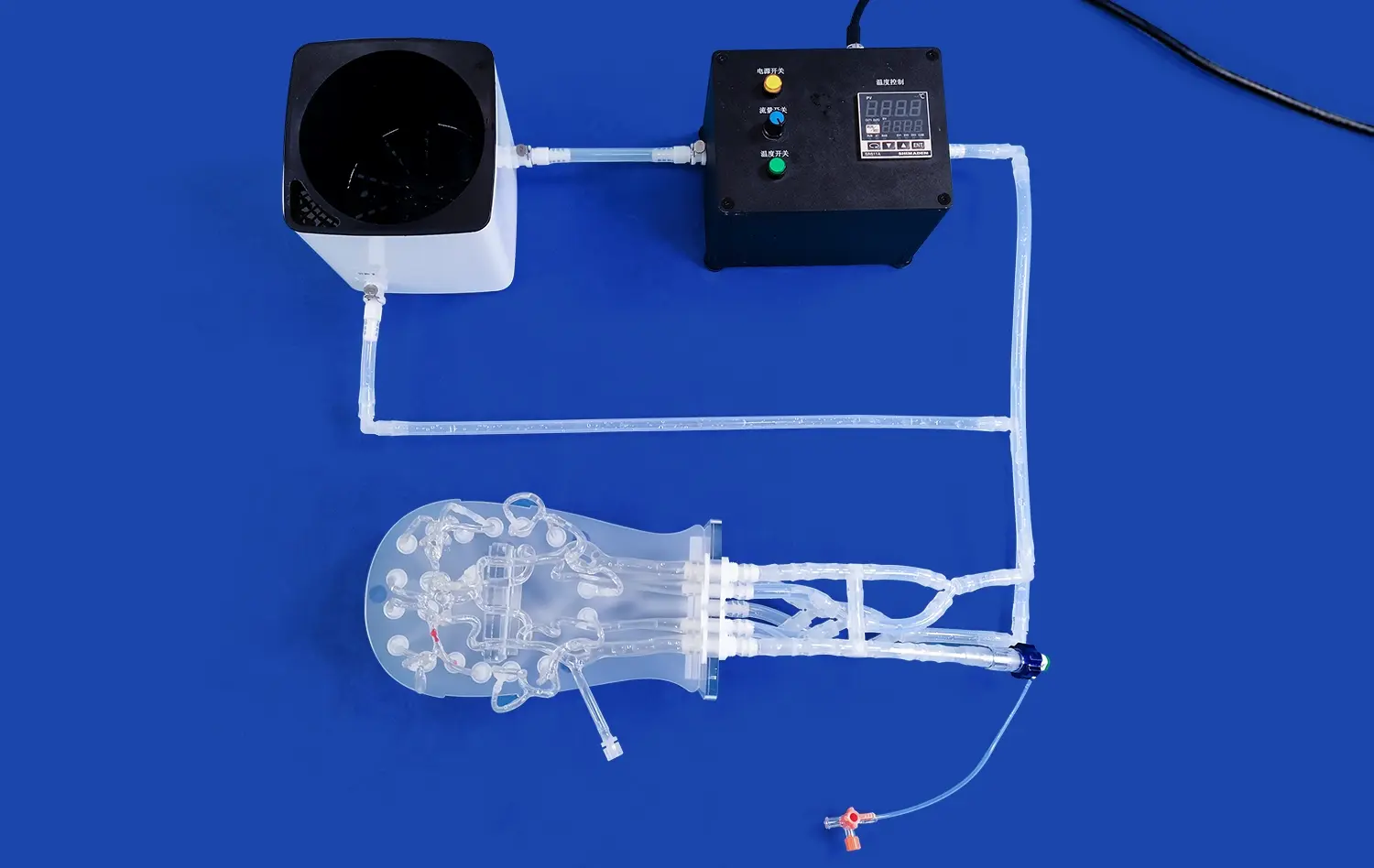
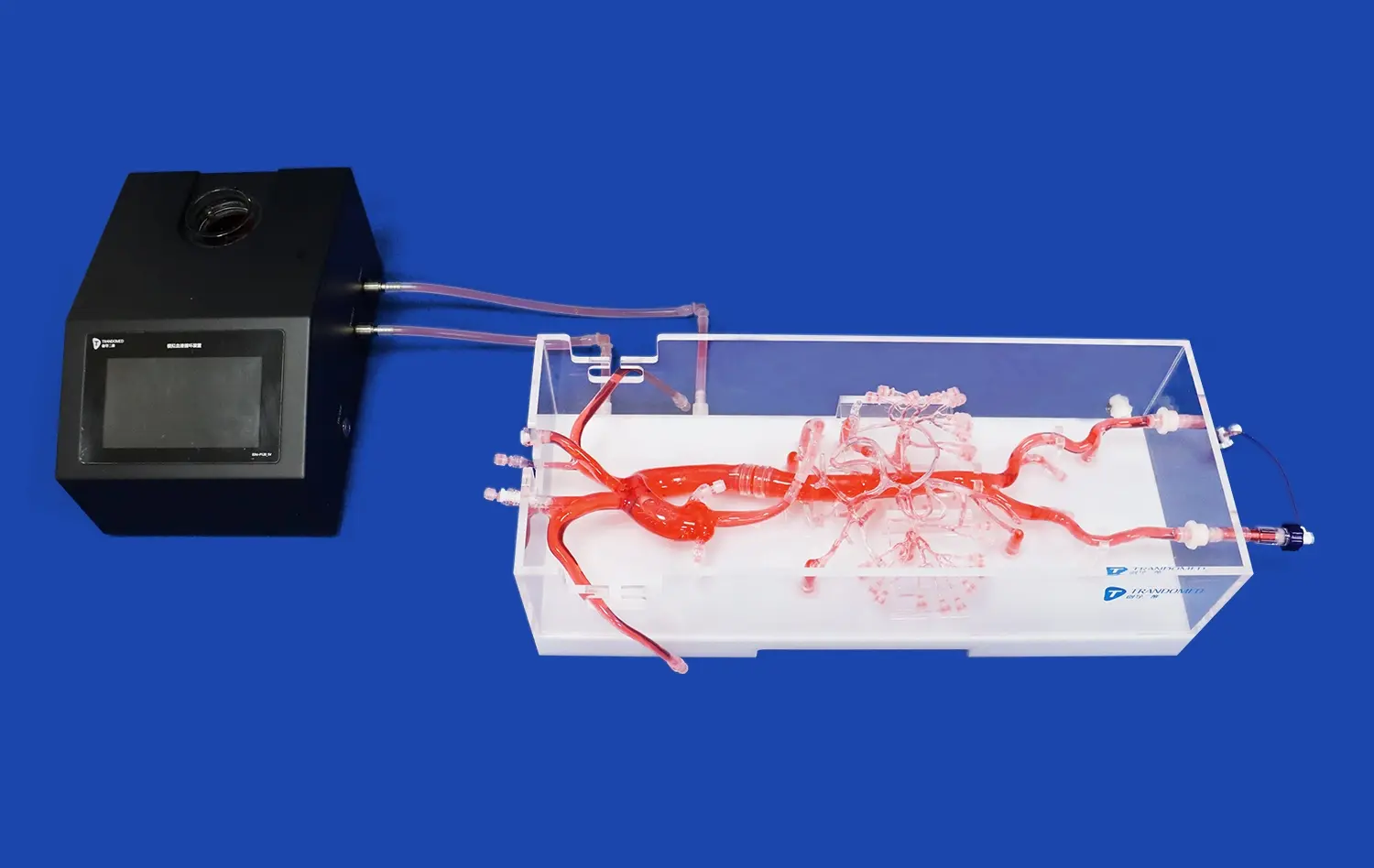
These days, exercise platforms are more than just static congenital heart disease intervention training models of bodies. Many of them use materials that are compatible with fluoroscopy, which lets multiple images be taken at the same time during simulated operations. Some high-tech systems have pressure monitors that give real-time feedback on how the catheter is being handled, while others connect to equipment that checks the patient's blood flow to mimic how the body would react. These engaging parts make learning more real by creating situations that are very similar to real clinical situations. This speeds up the development of skills.
Evolution and Effectiveness of CHD Intervention Training Techniques
Limitations of Traditional Training Approaches
In the past, pediatric cardiologists learned how to do invasive procedures by watching more experienced doctors do them and then gradually taking over their tasks. This method comes with some risks, since patients are used as test subjects, and some odd defects might not show up during training. While cadaveric dissection is useful for learning about anatomy, it can't show how a tube moves through living tissue or how a device interacts with it. In the past, these limitations have made training take longer and caused differences in the level of education across regions.
Simulation-Based Learning Advantages
Medical education research shows that training through simulations cuts down on mistakes and speeds up the learning process. Studies that compare traditionally trained cardiologists to those who were taught on a simulator show that simulator-trained cardiologists are better at handling catheters, using fluoroscopy, and making sure that devices are in the right place. Trainees say they feel more confident when they switch from computer practice to patient care. Being able to try new things, repeat steps, and learn from mistakes without fear of repercussions provides a sense of safety that helps people remember what they have learned.
Quantifiable Improvements in Clinical Outcomes
Institutions that use organized simulations in their lessons have seen impressive results. One multi-center study looked at the rate of complications before and after the simulator was added. They found that access-site complications went down by 34% and device changes for ASD closures done by newly trained interventionalists went down by 28%. Another study showed that fellows who did 20 simulator cases before they actually worked with patients became procedurally independent 6 months faster than their peers who only used traditional ways of training.
Standardization Across Training Programs
Standardizing the program is now possible with simulation models, which wasn't possible before. Training directors can set competency standards based on simulator performance measures. This way, all graduates meet the same skill levels, no matter what kinds of patients they see during their fellowship. When a rare defect shows up, this standardization is especially helpful. For example, trainees can practice different PDA configurations or muscular VSD closures on simulations, even if these cases never come up in their clinical shift.
Selecting the Best Congenital Heart Disease Intervention Training Model
Critical Evaluation Criteria
Anatomical accuracy should be the most important thing for procurement managers to look for in training simulations. For pediatric patients, models must properly show the sizes of vessels, the proportions of cardiac chambers, and the relationships between spaces. Not only static accuracy is important, but also functional realism. The model should be able to simulate moving a catheter, manipulating a guidewire, and deploying a device with force input that matches what happens in real life. Total cost of ownership is affected by durability, since training programs need models that can last through hundreds of practice sessions.
Customization Capabilities and Clinical Relevance
Because of the wide range of congenital heart defects, teaching tools need to be adaptable. Better models let you change the sizes and places of flaws, so teachers can make exact copies of patients' bodies to practice on before surgery. This method is shown by the Trandomed XXS003 model, which can be changed to fit each patient's needs using CT, CAD, or STL data files. Adding secondary pathologies, like ASD and PFO happening at the same time or VSD presentations that happen together, makes learning situations more complete and accurate to clinical complexity.
Institutions should think about their educational goals before choosing a training tool. In programs that focus on developing basic skills, simple, long-lasting models for repeated practice may be given more weight. Highly customizable simulators with rare defect presentations are helpful for advanced training schools that prepare interventionalists for difficult cases. Cost-benefit analysis should account for model lifespan, the number of concurrent trainees it can support, and whether its versatility eliminates the need for multiple specialized models.
Supplier Evaluation and Partnership Considerations
Picking the right provider is about more than just getting good products. Companies should be judged on how good they are at medical simulation by looking at their research and development (R&D) and clinical advice networks. Access to technical support is important because teachers need help figuring out how to use congenital heart disease intervention training models most effectively and follow maintenance procedures. Delivery times affect when programs are put into action, so it's important to have efficient logistics. Manufacturers that let you change the style of their products without charging extra are strategically advantageous because they let you change the curriculum without having to keep spending money on it.
Implementing Congenital Heart Disease Intervention Training in Your Organization
Curriculum Integration Strategies
Successful simulation programs require deliberate curricular design rather than ad hoc model access. Leading institutions embed simulator training within structured rotations, beginning with basic catheter skills before progressing to complete procedural sequences. Milestone-based advancement ensures trainees master foundational techniques before attempting complex interventions. Pairing simulator sessions with case-based discussions and imaging review creates multimodal learning that reinforces spatial understanding and decision-making processes.
Addressing Common Implementation Challenges
Budget constraints frequently emerge as implementation barriers. However, the cost analysis should consider avoided complications and reduced training time—simulator investment often proves economically favorable when accounting for these factors. Space limitations can be addressed through mobile simulation carts or shared-use scheduling with other procedural training programs. Faculty time commitment concerns diminish when institutions designate simulation champions who develop expertise in maximizing educational value from available models.
Measuring Training Effectiveness
Robust assessment frameworks validate simulation program value and identify improvement opportunities. Performance metrics might include procedural completion time, fluoroscopy duration proxies, device positioning accuracy, and complication recognition. Comparing these metrics across training cohorts reveals curriculum effectiveness. Post-training surveys capture learner confidence levels, while supervisory assessments during initial patient cases measure skill transfer. Tracking long-term clinical outcomes for simulator-trained versus traditionally trained cardiologists provides ultimate program validation.
Emerging Trends in Simulation Technology
The next generation of training tools incorporates artificial intelligence for personalized feedback and adaptive difficulty progression. Haptic feedback systems provide increasingly realistic tactile sensations, while augmented reality overlays can highlight anatomical structures during practice sessions. Connectivity features enable remote proctoring, allowing expert cardiologists to guide trainees across geographic distances. Staying informed about these developments helps organizations plan strategic upgrades that maintain training program competitiveness and effectiveness.
Procurement Guide: Purchasing Congenital Heart Disease Intervention Training Models
Needs Assessment Framework
Organizations should begin procurement by clearly defining their training population and objectives. Medical schools require different features than surgical training labs preparing experienced cardiologists for rare procedures. Anticipated annual trainee volume influences durability requirements and budget allocation. Understanding the specific defect types most relevant to your clinical practice—whether common ASDs or complex single-ventricle pathologies—guides model selection toward appropriate anatomical configurations.
Understanding the Investment Landscape
Training model investment ranges from basic anatomical replicas suitable for orientation to sophisticated hybrid systems integrating imaging and physiological simulation. Entry-level models provide excellent value for fundamental skill development, while advanced platforms justify their premium through expanded capabilities and longer functional lifespan. Procurement decisions should account for not just initial acquisition costs but also maintenance requirements, replacement component availability, and potential upgrade pathways that protect long-term investment value.
Vendor Partnership and Support Services
Working with established manufacturers brings advantages beyond product quality. Trandomed, with over 20 years specializing in medical 3D printing technology, exemplifies the expertise level that ensures product reliability. Their silicone Shore 40A models demonstrate material science sophistication that delivers clinical realism. The XXS003 congenital heart disease intervention training model's comprehensive vascular anatomy—from femoral access through atrial structures—reflects deep understanding of interventional workflows. Their 7-10 day delivery timelines and acceptance of customization without design fees represent the service flexibility that streamlines program implementation.
Quality Assurance and Regulatory Considerations
Medical simulation products should meet established industry standards, with manufacturing processes subject to quality control protocols. Verify that suppliers can provide material safety documentation and, where applicable, regulatory compliance certifications. Understanding product warranties and replacement policies protects against premature failure. For institutions with specific anatomical requirements, suppliers offering sample evaluation or demonstration units enable hands-on assessment before large-scale purchases.
Conclusion
Advancing pediatric cardiology training through high-fidelity simulation models represents a strategic investment in clinical excellence and patient safety. The evidence overwhelmingly supports simulation-based learning as superior to traditional apprenticeship models alone, offering repeatable practice without patient risk while accelerating competency development. Thoughtful model selection—prioritizing anatomical accuracy, customization capability, and supplier expertise—ensures training programs meet current needs while adapting to future requirements. By integrating these tools within structured curricula and measuring outcomes rigorously, medical institutions cultivate skilled interventionalists prepared to deliver optimal care for complex congenital heart conditions.
FAQ
What advantages do physical simulation models offer compared to traditional training methods?
Physical intervention training models provide risk-free environments where practitioners can repeat procedures until mastery is achieved, eliminating patient safety concerns during skill acquisition. Unlike patient-based learning, simulators allow deliberate practice of rare defect presentations and complication management. Trainees develop procedural confidence and muscle memory before encountering live cases, reducing anxiety and improving performance during actual interventions.
Can these training models integrate with telemedicine or remote learning platforms?
Many modern simulation programs successfully incorporate remote proctoring capabilities, where experienced cardiologists observe trainee performance via video connections and provide real-time guidance. While the physical models themselves remain at training facilities, recorded practice sessions can be reviewed asynchronously for feedback. Some institutions create hybrid programs combining simulator hands-on experience with virtual didactic sessions, expanding access to expert instruction regardless of geographical constraints.
How frequently should training models be updated or replaced?
Model replacement depends on usage intensity and material durability. High-quality silicone simulators like Trandomed's XXS003 withstand hundreds of practice sessions before showing significant wear. Institutions should establish inspection protocols monitoring for material degradation, anatomical distortion, or reduced fidelity. As clinical practices evolve or new defect presentations become training priorities, customization options allow model modification rather than complete replacement, optimizing resource utilization while maintaining educational relevance.
Partner with Trandomed for Advanced Pediatric Cardiac Training Solutions
Trandomed stands as your strategic congenital heart disease intervention training model supplier, bringing two decades of medical 3D printing innovation to simulation education. Our XXS003 model delivers the anatomical precision and material realism that accelerate trainee competency while ensuring patient safety during the learning curve. We accept customization requests across ASD dimensions, defect locations, and additional pathology integration—all without design fees—tailoring solutions to your specific educational requirements. With rapid 7-10 day production cycles and comprehensive technical support, we streamline implementation so your program launches efficiently. Contact jackson.chen@trandomed.com to discuss how our high-fidelity simulators can transform your pediatric cardiology training curriculum and position your institution at the forefront of interventional education excellence.
References
Anderson, J.M., & Roberts, K.L. (2021). Simulation-Based Training in Pediatric Cardiology: A Systematic Review of Educational Outcomes. Journal of Medical Education and Curricular Development, 8, 234-251.
Chen, W., Thompson, R.H., & Martinez, D.P. (2020). Three-Dimensional Printing Applications in Congenital Heart Disease: Current State and Future Directions. Pediatric Cardiology Review, 15(3), 142-158.
Hamilton, S.R., & Davidson, M.J. (2022). Cost-Effectiveness Analysis of Simulation Training for Interventional Cardiology Procedures. Health Economics and Medical Education Quarterly, 29(4), 567-582.
Liu, Y., Patterson, G.K., & Johnson, A.M. (2019). Anatomical Fidelity in Medical Simulation Models: Materials Science and Clinical Realism. Journal of Biomedical Materials Research Part B, 107(6), 1893-1907.
Patel, N.S., & Williams, C.T. (2023). Competency-Based Training Models in Pediatric Interventional Cardiology: A Multi-Institutional Study. Circulation: Cardiovascular Interventions, 16(2), e012456.
Zhang, L., Morrison, K.W., & Sullivan, P.R. (2021). Impact of High-Fidelity Simulation Training on Procedural Outcomes in Congenital Heart Disease Interventions. American Journal of Cardiology Education, 34(1), 78-94.