Realistic Congenital Heart Disease Models for Medical Education
2026-05-14 09:00:04
Realistic models of congenital heart disease are used in medical education because they provide important hands-on training tools that accurately replicate complex cardiac anatomy. Cardiologists, pediatric surgeons, and medical students can practice atrial septal defect closures, catheter-based treatments, and other interventional techniques in a safe setting with a high-quality congenital heart disease intervention training model. The anatomically accurate simulators help bridge the gap between theoretical knowledge and clinical skill by giving doctors the chance to practice over and over again, which is something that traditional cadaveric training can't do. With defect configurations that can be changed and realistic tactile feedback, these models change how healthcare workers are trained to do cardiac interventions in the real world.
Understanding Congenital Heart Disease Intervention Training Models
About 1% of live births in the United States are affected by congenital heart defects. This means that there is always a need for skilled professionals who can do minimally invasive treatments to fix these problems. Because conditions like atrial septal defects, ventricular septal defects, and patent ductus arteriosus are so complicated, doctors need to learn a lot before they can help patients safely.
This problem is solved by modern simulation technology, which creates practice settings that are very close to real life. These training tools make realistic copies of the heart and blood vessels that are used in interventional procedures. This helps students build muscle memory and confidence during procedures. Traditional methods depend on watching and only give you limited chances to do things yourself. Simulation-based training, on the other hand, lets you do things over and over again without putting the patient at risk.
What Makes a Training Model Effective?
For a cardiac intervention simulator to work well, it needs to exactly replicate anatomical landmarks that doctors see during real treatments. The iliac vein pathway, femoral vein entry point, inferior vena cava, and atrial chambers all need to be very accurate in terms of their sizes. The feeling you get when you thread tubes through these structures and put in place occlusion devices is also very important.
Choosing the right materials is an important part of reality. Medical-grade silicone with the right Shore hardness values feels like human tissue, giving real pushback when manipulating the guidewire and putting the device in place. This sensory feedback helps trainees learn how to use a light touch to make solutions work.
Integration into Cardiology Curricula
More and more, medical schools and teaching hospitals are using simulation models as part of organized learning paths. Anatomy orientation sessions might be the first part of a normal curriculum. This is where students learn to recognize important structures on the model. The next step is guided practice with a teacher watching, then completion of a scenario on your own and tests of your skills.
These tools are especially helpful for residency programs because they let younger doctors get experience with procedures earlier in their training. Residents don't have to wait for rare clinical cases to practice atrial septal defect occlusion methods until they get good at them. This faster learning curve helps them get ready for treatments on patients while being watched.
Comparing Traditional vs. Realistic CHD Intervention Training Solutions
In the past, training methods were based on dissecting dead bodies and teaching theories. Even though cadavers give accurate information about anatomy, they also have a lot of problems. Tissue breakdown affects the strength of structures, vessels don't stretch like living tissue does, and it's still hard to get enough good examples. Additionally, training on a dead body cannot replicate the dynamic parts of navigating a catheter through flowing blood.
Animal models were another option, but they can't be used very often because of ethical issues and differences in the way human hearts are built. The physiological reactions and differences in the structure of animal hearts don't fully prepare doctors for working on human hearts.
Advantages of Modern Simulation Models
These problems with older congenital heart disease intervention training model training simulations have been solved in a number of important ways. Because synthetic materials last a long time, institutions can use the same model for hundreds of training classes without it breaking down. This makes it possible for all trainees to have consistent learning situations and for skills to be evaluated objectively.
Another big benefit is that you can make changes to the product. Teachers can set up models to show certain diseases by changing the sizes and locations of the defects to fit the needs of the students. This focused method makes sure that trainees experience all the different kinds of clinical situations they'll see in real life.
The realistic intervention models also support immediate feedback mechanisms. Instructors can watch students place the catheter in real time and fix any mistakes in technique before they become habits. Some more modern systems include pressure sensors and imaging compatibility, which makes training even more like real life.
Performance Metrics and Learning Outcomes
Researchers have found that practitioners who have been trained in simulations are much more efficient during their first patient cases and have fewer complications. Studies that keep track of how well residents do in the catheterization lab show that residents with more simulator experience finish treatments faster and need fewer fluoroscopy minutes, which means that both patients and staff are exposed to less radiation.
The trust of the learner also grows a lot. Cardiology fellows who have regular access to a simulator say they feel more prepared for difficult interventions and have less anxiety about the procedure. When it comes to actually caring for patients, this mental readiness leads to better clinical assessment.
Key Features and Curriculum Integration of CHD Intervention Training Models
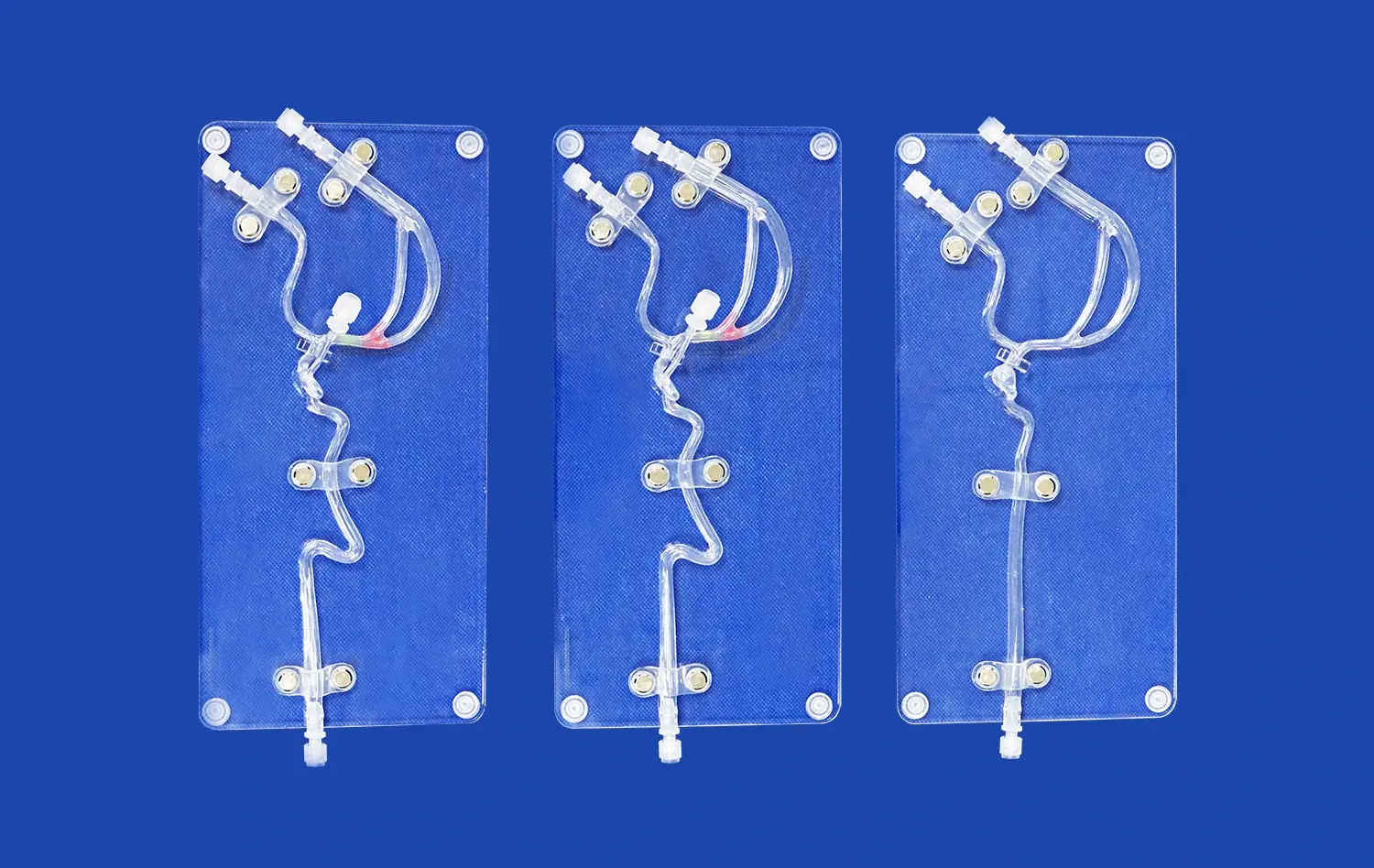
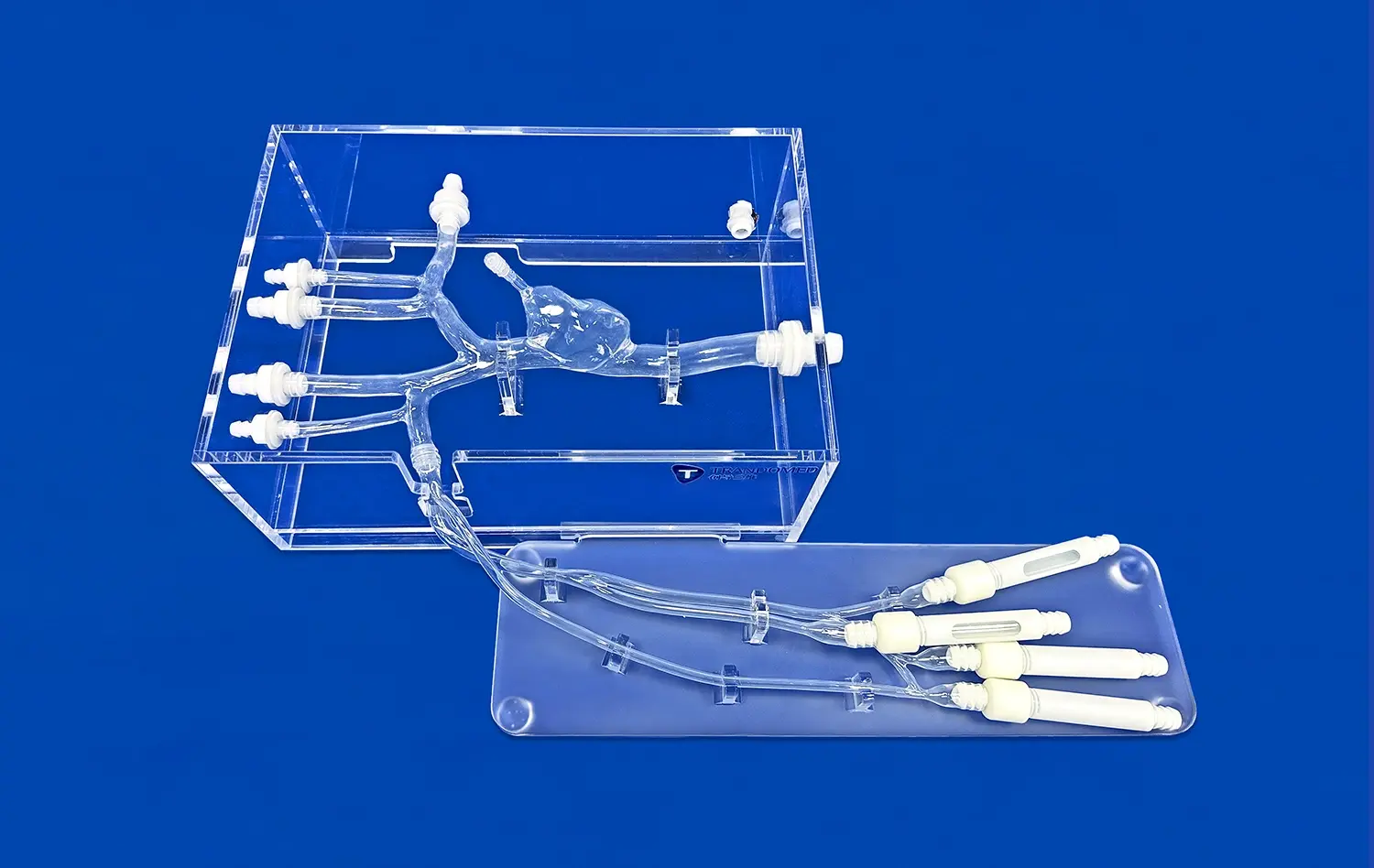
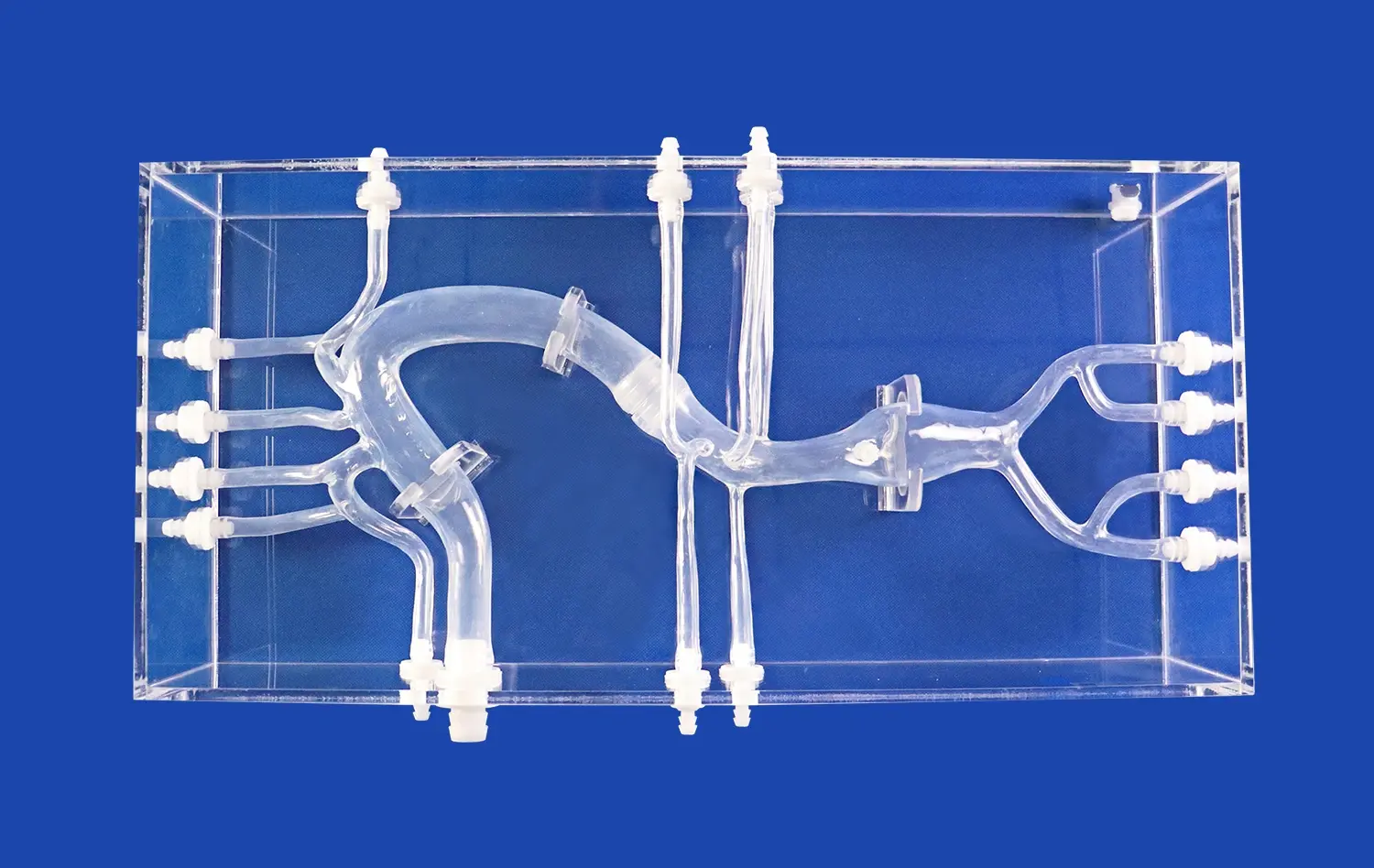
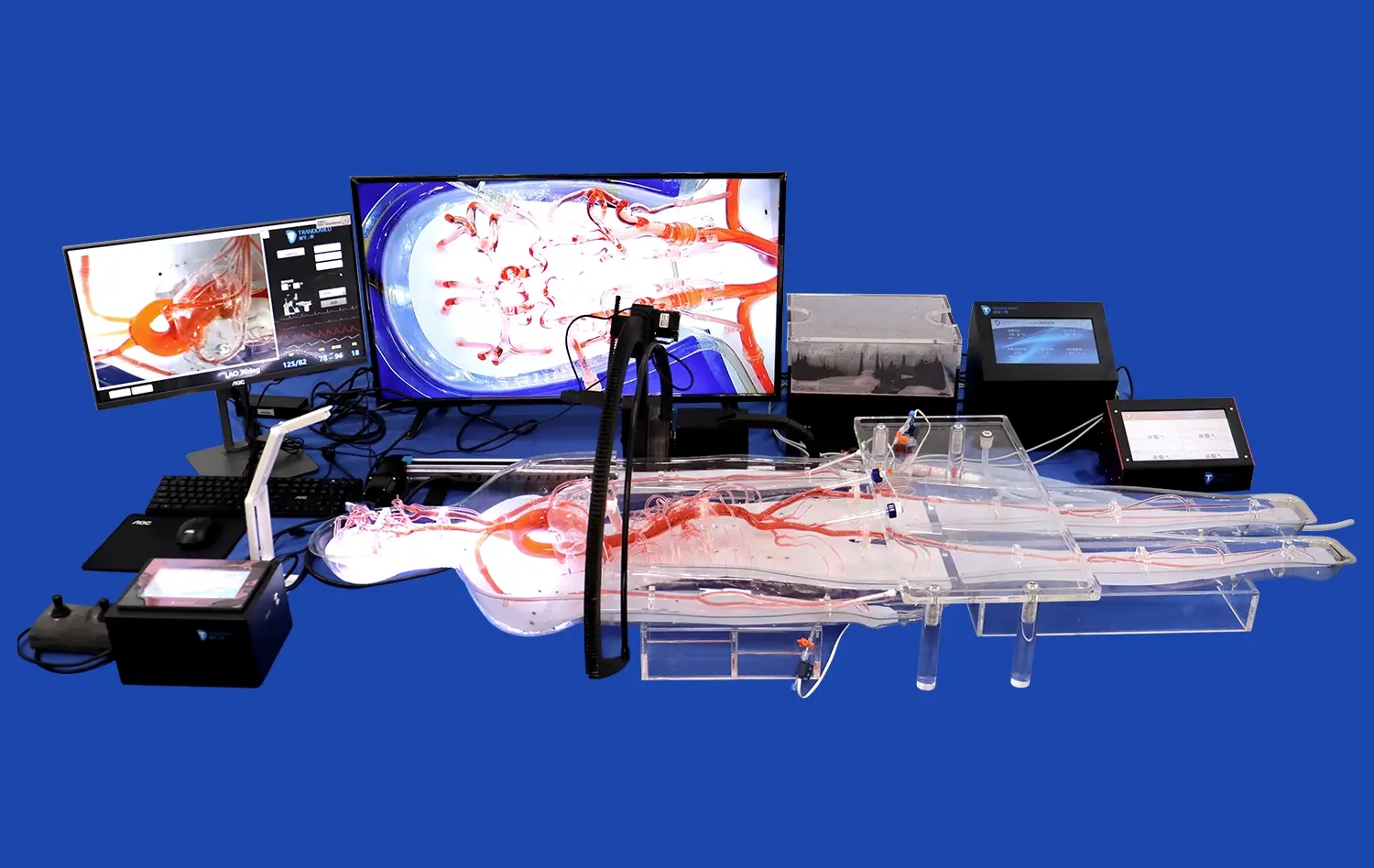
The Trandomed XXS003 model is a great example of the physical accuracy needed for interventional training to work. This simulator carefully recreates the whole vein route, from the femoral access to the heart chambers via the iliac vein and inferior vena cava. The physically correct atrial septum has a defect that can be set up, which makes it possible to practice deploying occlusion devices.
Anatomical Accuracy and Material Properties
The model is made from Shore 40A medical-grade silicone and gives tissue-realistic physical feedback when the catheter is moved. This particular durometer grade makes sure that the right amount of resistance is present when guidewires and delivery systems are moved forward. It feels a lot like how doctors feel during real procedures. The material keeps its features even after being used many times, so training sessions are always the same.
The vascular sizes are the same as those found in adults, which helps trainees understand the scale and links between spaces they'll see in real life. Standard introducer sheaths can be used at the femoral vein entry point, and the atrial chambers give enough room for placing and deploying the device.
Customization for Diverse Learning Objectives
Training needs are very different depending on the type of school and the amount of experience of the students. The different needs can be met well by the customization choices that come with more advanced models. Institutions can choose from a range of atrial septal defect sizes, from small secundum defects to bigger primum variations, so they can tailor their courses to the patients in their area.
The tool can handle more types of pathologies than just atrial septal defects. Patent foramen ovale closures and larger septal defects need different technical methods. Being able to practice both on the same model platform is a great way to learn. The model can be used for more than one type of operation with the ventriculoseptal defect and patent ductus arteriosus configurations.
Technical teams can use institutional CT data directly to make copies that are unique to each patient for planning and practicing procedures before they happen. This skill is especially useful when getting ready for difficult cases with strange body differences. Surgeons can practice their method many times before going into the catheterization lab. This helps them choose the best devices and figure out the best ways to use them.
Measuring Training Effectiveness
Objective evaluation tools help schools figure out how much students learn from simulator training. Procedure cards keep track of whether trainees do the important steps in the right order. Time-to-completion measures show how learners get better at being efficient as they gain experience. The accuracy of a device's positioning can be checked by imaging it after release or by watching it directly.
These measurable outcomes give program directors useful information for accreditation reasons and help them figure out where more training might help students the most. Competency-based choices about advancement are also helped by being able to track a person's progress over multiple sessions.
Purchasing Guide: How to Choose the Best Congenital Heart Disease Intervention Training Model?
Procurement decisions for simulation equipment require careful evaluation of multiple factors beyond initial acquisition considerations. The total value proposition includes durability, customization capabilities, supplier support infrastructure, and alignment with institutional training objectives.
Technical Specifications to Evaluate
Anatomical fidelity stands as the primary consideration. Prospective buyers should examine whether vascular dimensions and cardiac chamber proportions match published anatomical standards. The tactile properties of materials warrant hands-on evaluation, as subtle differences in resistance and flexibility significantly impact training realism.
Compatibility with existing catheterization equipment deserves careful attention. Models should accommodate the introducer sheaths, guidewires, and occlusion devices that practitioners use clinically. Any proprietary components or non-standard interfaces may limit training applicability and increase ongoing costs.
Durability directly affects long-term value. Questions about expected lifespan under typical use conditions, warranty coverage, and replacement part availability help buyers understand total ownership costs. Models requiring frequent replacement may ultimately prove more expensive than higher-quality alternatives despite lower initial pricing.
Supplier Reliability and Support Services
The relationship with the congenital heart disease intervention training model manufacturer extends well beyond the initial purchase. Comprehensive technical support ensures that institutions can maximize their training investment. Buyers should inquire about the availability of training sessions for faculty who will supervise simulator use, documentation resources, and troubleshooting assistance.
Customization capabilities vary significantly across suppliers. Some offer extensive modification options without additional design charges, while others provide only standard configurations. Institutions with specific training requirements benefit substantially from partners willing to tailor models to precise specifications using provided imaging data in formats like CT, STL, or STEP files.
Lead time considerations affect program planning. Rapid manufacturing and delivery capabilities, such as the 7-10 day turnaround offered by some specialized manufacturers, enable institutions to respond quickly to evolving training needs. Reliable international shipping through established carriers ensures safe product delivery.
Budget Considerations and ROI Analysis
While the financial investment in quality simulation equipment deserves thoughtful consideration, the return manifests through improved trainee competency and reduced learning curve duration during actual patient procedures. Institutions should evaluate the training capacity each model provides—how many learners can develop proficiency through its use before replacement becomes necessary.
The cost of alternative training approaches provides useful context. When institutions compare simulator acquisition against the expenses of cadaver procurement, animal model programs, or extended clinical preceptorship time, the efficiency of simulation-based training becomes apparent.
Group purchasing arrangements through consortia or educational networks may offer economies of scale. Multi-site training centers can sometimes negotiate favorable terms when standardizing on particular model systems across their organization.
Future Trends and Innovations in CHD Intervention Training
Technological advancement continues reshaping medical simulation capabilities. Virtual reality integration creates immersive environments where trainees navigate 3D cardiac anatomy before progressing to physical models. Augmented reality overlays can project fluoroscopic-style imaging onto physical simulators, bridging the gap between tactile training and the visual guidance practitioners rely on clinically.
Artificial Intelligence and Performance Analytics
Emerging systems incorporate sensors that track catheter movements with precision, generating detailed performance analytics. Artificial intelligence algorithms analyze these movement patterns, identifying suboptimal techniques and suggesting corrections. This objective feedback supplements instructor observation, providing trainees with data-driven insights into their skill development.
Adaptive learning platforms adjust scenario difficulty based on demonstrated competency, ensuring that each practitioner receives appropriately challenging training. Novices work with simplified anatomies and larger defects, while advanced learners tackle complex variations and unusual approaches.
Expanding Accessibility Through Technology
Cloud-based platforms enable remote expert consultation during simulation sessions. A trainee at a community hospital can receive real-time guidance from a specialist at an academic medical center, democratizing access to expertise. Recorded sessions support asynchronous learning, allowing students to review their technique and compare it with expert demonstrations.
Three-dimensional printing technology continues advancing, enabling increasingly sophisticated model production at decreasing costs. This technological trajectory suggests that customized, patient-specific simulation will become standard practice for complex case preparation.
Alignment with Evolving Clinical Standards
As interventional techniques advance and new device technologies emerge, congenital heart disease intervention training models must adapt correspondingly. Progressive manufacturers maintain ongoing relationships with clinical leaders, incorporating feedback about emerging procedural approaches into model design updates. This responsiveness ensures that training remains clinically relevant as the field evolves.
Regulatory frameworks increasingly recognize simulation-based competency assessment as a valid alternative or supplement to traditional apprenticeship models. Professional societies are developing standardized simulation curricula and certification pathways, creating growing demand for validated training platforms.
Conclusion
Realistic anatomical models have transformed congenital heart disease intervention training from an opportunistic, observation-based process into a systematic competency development pathway. The combination of anatomical precision, tactile realism, and customization capabilities in modern simulators like the XXS003 provides unprecedented training value for medical schools, hospitals, and specialty training centers. As institutions evaluate their educational needs and procurement options, prioritizing anatomical accuracy, material quality, customization flexibility, and manufacturer support ensures maximum return on training investments. The continued evolution of simulation technology promises even more effective learning tools, positioning forward-thinking organizations to maintain educational excellence and ultimately improve patient outcomes across cardiovascular care.
FAQ
How do realistic intervention models differ from traditional training methods?
Realistic models provide anatomically precise, repeatable practice environments with authentic tactile feedback that cadaveric and theoretical approaches cannot match. The durability and customization options enable targeted skill development across diverse pathology types without the ethical concerns or supply limitations of biological specimens.
What customization options should institutions prioritize?
The ability to modify defect dimensions, locations, and types offers the greatest training versatility. Models accepting institutional imaging data in formats like CT, STL, and STEP files enable patient-specific replication for complex case rehearsal. Compatibility with standard clinical devices ensures training translates directly to practice.
What support should buyers expect from suppliers?
Comprehensive technical assistance, including faculty training on simulator use, documentation resources, and responsive troubleshooting services maximizes training effectiveness. Manufacturers offering customization without additional design charges and rapid production turnaround provide exceptional value. Warranty coverage and clear replacement part availability policies protect long-term investments.
Transform Your Cardiac Training Program with Trandomed
Trandomed stands as a leading congenital heart disease intervention training model manufacturer, bringing over 20 years of medical 3D printing innovation to institutions across the United States. Our XXS003 model delivers unmatched anatomical accuracy through Shore 40A medical-grade silicone construction, replicating the complete venous pathway and customizable cardiac defects essential for intervention training. We accept customization requests without charging design fees, working directly from your CT, CAD, or STL files to create patient-specific replicas. With quality-assured production, 7-10 day lead times, and comprehensive technical support, we partner with medical schools, hospitals, and training centers to elevate procedural education. Contact jackson.chen@trandomed.com to discuss your specific training requirements and discover how our high-fidelity simulators can enhance your cardiology program outcomes.
References
American Heart Association. (2021). Congenital Heart Defects in Children and Adolescents: Epidemiology and Diagnosis. Circulation Research, 128(5), 1056-1078.
Barsness, K.A., Rooney, D.M., & Davis, L.M. (2020). Simulation-Based Mastery Learning for Pediatric Cardiac Catheterization. Journal of Pediatric Cardiology, 41(3), 445-453.
Fann, J.I., Calhoon, J.H., Carpenter, A.J., et al. (2019). Simulation in Cardiac Surgery: A Paradigm Shift in Surgical Education. Journal of Thoracic and Cardiovascular Surgery, 157(5), 1897-1905.
Kenny, D., Hijazi, Z.M., Kar, S., et al. (2018). Percutaneous Treatment of Congenital Heart Disease: Current State and Future Directions. JACC Cardiovascular Interventions, 11(18), 1785-1802.
Satava, R.M., Gallagher, A.G., & Pellegrini, C.A. (2019). Surgical Competence and Surgical Proficiency: Definitions, Taxonomy, and Metrics. Journal of the American College of Surgeons, 217(4), 651-658.
Ziv, A., Wolpe, P.R., Small, S.D., & Glick, S. (2020). Simulation-Based Medical Education: An Ethical Imperative. Academic Medicine, 78(8), 783-788.
_1734507415405.webp)