Realistic Left Atrial Appendage Occlusion Training for Physicians
2026-05-21 09:00:04
Left atrial appendage occlusion has become an important way to keep people with atrial fibrillation from having a stroke. However, getting good at this delicate treatment takes a lot of practice in settings that are like real clinical settings. With a left atrial appendage closure simulator, doctors can get better at what they do without putting patients at extra risk. These advanced training models accurately mimic the complicated heart anatomy. This lets doctors practice guiding catheters, putting devices in place, and handling complications over and over again until they are experts at the procedure.
Understanding Left Atrial Appendage Anatomy and Closure Procedures
What Is the Left Atrial Appendage?
The small muscle pouch that sticks out from the left atrium of the heart is called the left atrial appendage. It looks like a finger and is close to the open wall of the left ventricle inside the pericardium. Even though it's small, the LAA is an important part of heart health because it releases natriuretic peptides that help keep blood volume stable when blood flow changes. Even though these processes are normal, the LAA has problems in people with atrial fibrillation because it is the main place where thrombi form, which is where over 90% of stroke-causing clots happen in this group of people.
The Four Main LAA Morphologies
Cardiologists have identified four main types of LAA shapes: chicken wing, cactus, windsock, and cauliflower. These were based on extensive imaging studies of groups of patients. As many as 48% of patients have the chicken wing shape, which is characterized by a prominent bend that makes closure operations more difficult. 30% of people have the cactus type, which has many lobes that go in different directions. In 19% of cases, the windsock morphology shows a single main lobe with a steady width. The cauliflower type is the strangest (only 3% of cases), and it has irregular, multilobular structures that are the hardest to treat.
Why Left Atrial Appendage Closure Matters?
By getting rid of the main cause of cardiac thrombus formation, left atrial appendage closure lowers the risk of stroke that comes with atrial fibrillation. While this procedure does not treat atrial fibrillation, it does lower the chance of stroke by a large amount by blocking the LAA. This intervention is perfect for people who can't take long-term anticoagulation therapy because they are at risk of bleeding, can't handle the medicine, or have living issues that make it impossible for them to do so. The procedure is an option to taking blood thinners for life, such as warfarin, apixaban, rivaroxaban, or dabigatran. It protects against thromboembolic strokes over time and doesn't require daily medication or bleeding problems.
Benefits of Using Simulation Technology in LAA Closure Training
Simulation-based training changes the way doctors learn how to do complicated heart procedures. Traditional ways of training, like corpse labs and proctored live cases, have big problems with being able to repeat the training, making it easy for people to get to, and keeping patients safe. Modern simulators get around these problems by making training situations that are standardized, repeatable, and suitable for people with different levels of skill.
Through controlled, risk-free practice settings, simulation training boosts doctors' confidence. Trainees can do procedures more than once to try out different methods and experience rare problems that don't affect patients. Compared to traditional ways, this repeated practice speeds up the learning curve by a large amount. Interventional cardiology studies have shown that doctors who have been trained in simulations reach procedural goals faster and with fewer problems during their first supervised cases.
Advanced simulations have objective performance tracking features that help institutions. These systems keep track of procedural measures like how well the catheter is handled, how long the fluoroscopy takes, how accurately the device is placed, and how quickly complications are identified. Training leaders can find specific skill gaps and make sure that students learn how to fix them. This method, which is based on data, makes competency standards that can be measured and help with choices about certification paths and credentials.
Simulator-based training is clearly the most cost-effective option when you look at the other options. For cadaver labs to work, they need expensive buildings, it can be hard to get and store specimens, and there are only so many chances to learn from each specimen. Concerns about ethics come up with live animal models, which need special sites and have high ongoing costs. Even though they require an initial input of money, left atrial appendage closure simulators allow for unlimited training repetitions with low ongoing costs. This makes them a good financial choice for institutions that want to run long-term training programs.
How to Choose the Best Simulator for Your Institution?
Evaluating Anatomical Accuracy and Realism
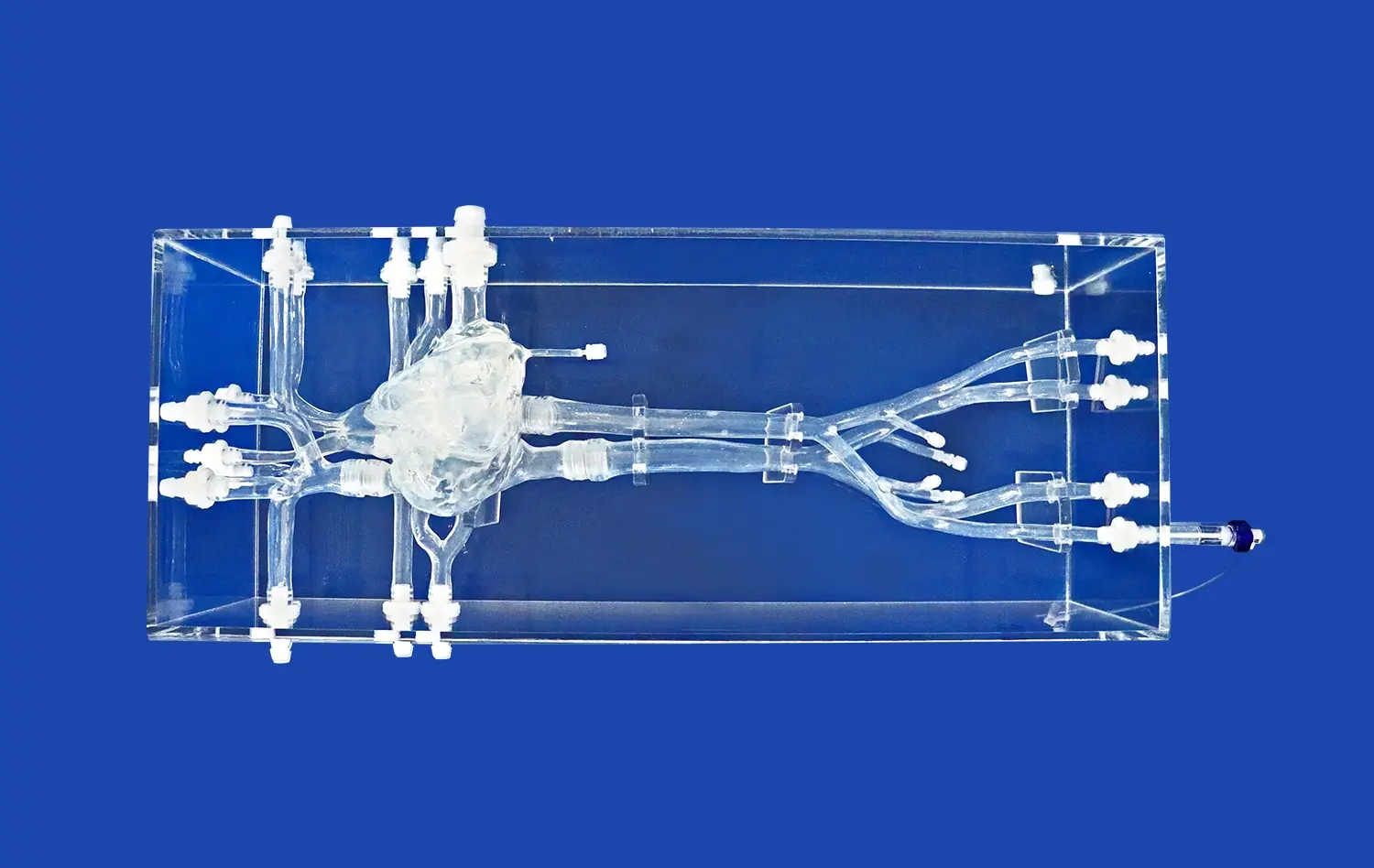
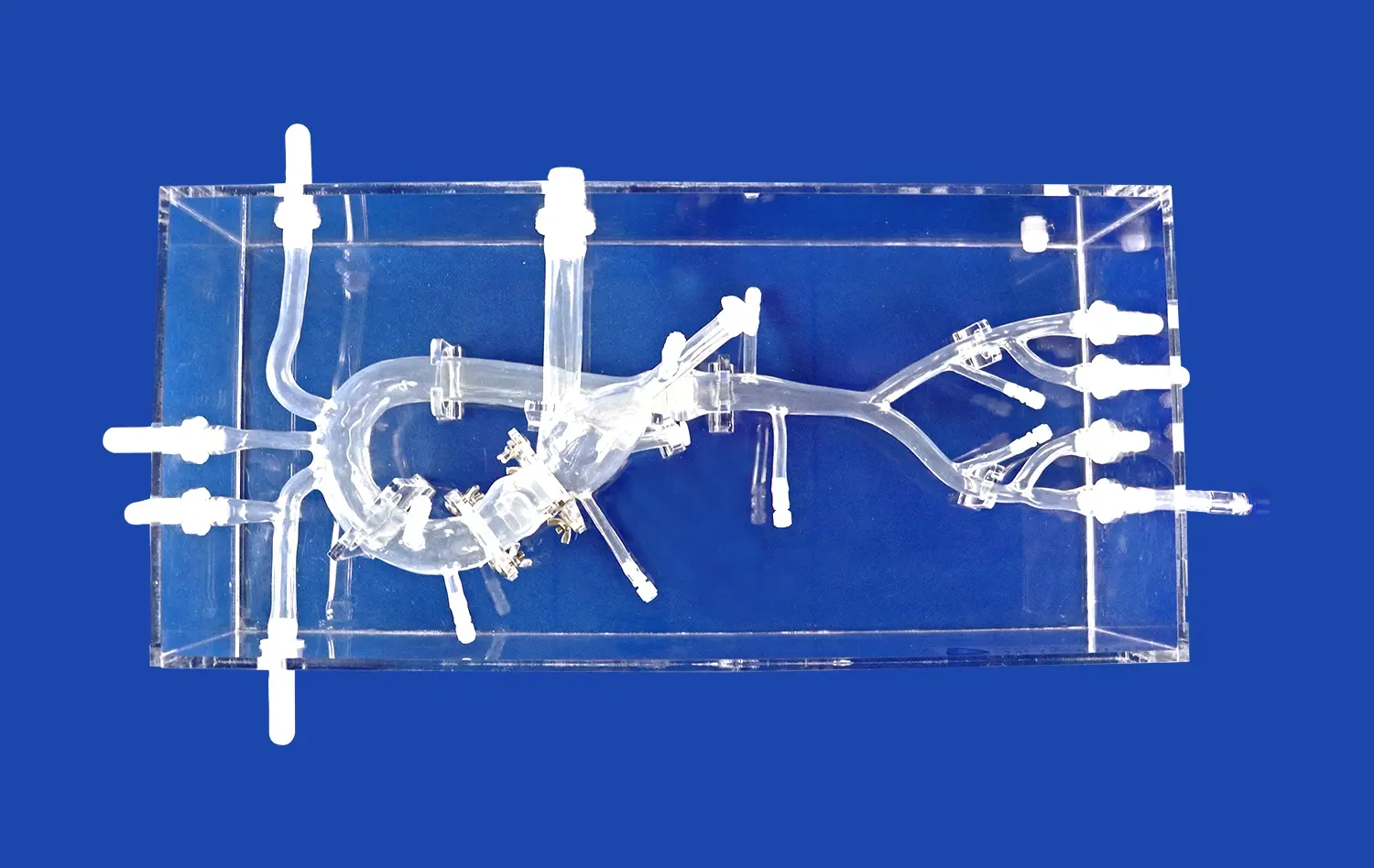
When choosing a training simulator, anatomical accuracy is the most important thing to think about. The device has to exactly copy the heart's structures from the femoral vein access point to the inferior vena cava, right atrium, atrial septum, left atrium, and most importantly, the left atrial appendage. The Trandomed Left Atrial Appendage Closure Simulator (XX013D) is a good example of this all-around method because it carefully recreates the whole procedure pathway, which includes the iliac vein, the inferior vena cava, both atria, the left atrial appendage, and the pulmonary veins.
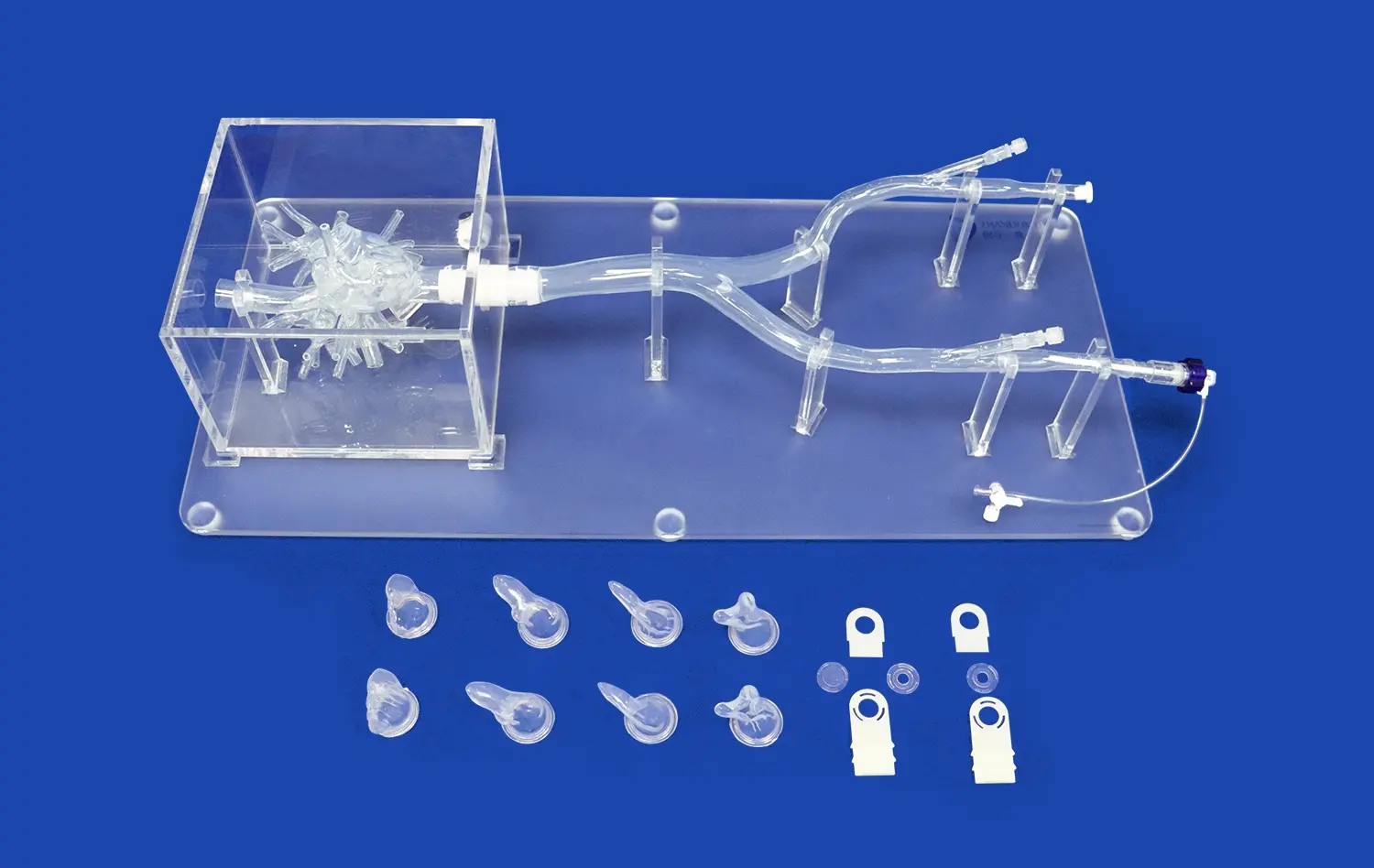
Most of the better models include all four types of LAA morphology, so students can get practice with all the different body types they will see in real life. The XX013D model comes in chicken wing, cactus, windsock, and cauliflower shapes, so you can practice both common and difficult body parts. This variety in shape is important because device selection and placement methods are very different depending on the shape of the LAA.
Material Properties and Tactile Feedback
The materials used to build the model have a direct effect on how well training works. Silicone mixtures with Shore hardness scores between 30A and 50A most closely match the properties of heart tissue. The XX013D is made of Shore 40A silicone, which gives accurate feedback when manipulating the tube, making a transseptal puncture, or deploying the device. This material helps doctors develop the right level of tactile awareness, which is necessary for finding anatomical landmarks, spotting resistance that means the patient is not properly positioned, and avoiding perforation.
Realistic haptic feedback helps trainees learn the fine touch needed for safe catheter handling. Too much force during transseptal puncture can cause a heart perforation, and not enough force can make it impossible to get in. Doctors can fine-tune their skills before working with patients by practicing on models made of the right materials.
Modular Design and Customization Capabilities
Training programs benefit tremendously from simulators offering modular, replaceable components. The XX013D features three replaceable atrial septal defects of varying sizes, enabling practice in both standard transseptal puncture and scenarios involving patent foramen ovale or existing septal abnormalities. This modularity extends the simulator's educational utility while reducing long-term costs since individual components can be replaced rather than purchasing entirely new systems.
Customization capabilities elevate simulators from general training tools to institution-specific educational assets. Trandomed accepts data files in multiple formats—CT, CAD, STL, STP, and STEP—allowing production of patient-specific models derived from actual clinical imaging. This capability proves invaluable for preoperative planning, device company demonstrations, and research applications. Institutions can request modifications to ASD location and dimensions at no additional design cost, ensuring the simulator aligns perfectly with specific training objectives.
Technical Support and Delivery Considerations
Procurement professionals must evaluate the complete ownership experience beyond initial purchase. Reliable manufacturers provide comprehensive after-sales support including technical assistance, replacement part availability, and training on optimal simulator utilization. Trandomed offers expedited production with seven to ten-day lead times and ships globally through established carriers including FedEx, DHL, EMS, UPS, and TNT, ensuring training programs experience minimal delays between ordering and implementation.
Implementing Simulator-Based LAA Closure Training Programs
Infrastructure and Space Requirements
Successful simulator integration begins with appropriate physical space allocation. Training areas should accommodate the simulator itself, fluoroscopy simulation equipment when applicable, and sufficient room for multiple observers during educational sessions. The compact design of physical simulators like the XX013D makes them suitable for standard procedure rooms, simulation centers, or dedicated training laboratories without requiring extensive facility modifications.
Technical support infrastructure deserves careful consideration. Designating staff members responsible for left atrial appendage closure simulator setup, maintenance, and troubleshooting ensures consistent availability for training activities. Establishing inventory systems for replacement components prevents training interruptions when consumable parts require replacement.
Curriculum Integration and Learning Objectives
Effective training programs establish clear learning objectives mapped to procedural competency milestones. Introductory sessions might focus on femoral access, catheter navigation through venous anatomy, and transseptal puncture technique. Intermediate training advances to LAA anatomy recognition across different morphologies, device sizing decisions, and deployment techniques. Advanced modules address complication recognition and management, including pericardial effusion, device embolization, and incomplete LAA sealing.
Structured curricula should incorporate objective assessment metrics that track trainee progression. Performance benchmarks might include procedure completion time, fluoroscopy duration, successful device deployment rate, and complication occurrence frequency during simulated cases. These metrics provide tangible evidence of competency development and inform decisions about advancement to proctored clinical cases.
Case Studies Demonstrating Training Effectiveness
Medical education institutions implementing comprehensive simulation programs report measurable improvements in physician competency and patient outcomes. Teaching hospitals integrating LAA closure simulators into interventional cardiology fellowships observe fellows achieving independent practitioner status with fewer proctored cases than historically required. The ability to practice extensively on simulators before performing initial patient procedures reduces anxiety, enhances technical proficiency, and improves patient safety metrics.
Device manufacturers have discovered that physician training on simulators accelerates new product adoption. When cardiologists gain hands-on experience with closure devices in simulated environments, they develop greater confidence in the technology and more readily incorporate these procedures into their clinical practice. This benefit extends beyond individual physician training to support institutional program development, particularly for centers establishing new structural heart programs.
Future Trends and Innovations in LAA Occlusion Simulation
Artificial Intelligence and Adaptive Learning
Emerging artificial intelligence applications promise to revolutionize simulation training through adaptive learning algorithms. Future simulators may analyze individual trainee performance in real-time, automatically adjusting scenario difficulty and providing personalized feedback targeting specific skill deficiencies. Machine learning systems could identify subtle patterns in catheter handling that correlate with procedural success, offering insights that accelerate skill acquisition beyond what traditional instruction provides.
Expanded Anatomical Variants and Pediatric Applications
To meet the needs of specific training, the simulator market keeps growing. As more people learn that there are more than four main types of LAA morphologies, the need for models that include rare configurations and pathological anatomy grows. Pediatric cardiac intervention training is another new area of use, though LAA closure is still mostly an adult treatment because of how atrial fibrillation works.
Integration with Clinical Guidelines
Institutions that are looking to the future know that simulators need to change along with clinical practice standards and device technology. Training tools will still be useful as new closing devices come out and procedures get better because they are made in a way that lets parts be updated. Partnerships between companies that make simulators and companies that make devices make it easier to quickly adapt to changes in the industry. This protects institutional training investments over long periods of time.
Conclusion
Realistic simulation training has become indispensable for developing physician competency in left atrial appendage occlusion procedures. High-fidelity models like the Trandomed XX013D left atrial appendage closure simulator provide comprehensive training environments that replicate anatomical complexity while eliminating patient risk. The inclusion of multiple LAA morphologies, replaceable atrial septal components, and customization capabilities addresses diverse educational needs across medical schools, hospital training departments, and device manufacturers. As healthcare institutions face increasing pressure to ensure procedural competency while maintaining patient safety, simulation-based training offers a proven, cost-effective solution that enhances clinical outcomes and accelerates physician development.
FAQ
How Accurate Are Simulators Compared to Actual Procedures?
Modern high-fidelity simulators replicate anatomical structures and procedural steps with remarkable precision. The XX013D simulator reproduces the complete venous pathway from femoral access through cardiac chambers using silicone materials that mimic tissue properties encountered during actual procedures. While simulators cannot perfectly duplicate every aspect of live patient anatomy—including natural tissue variations and real-time physiological responses—they provide sufficient realism for developing fundamental technical skills that transfer effectively to clinical practice. Research comparing simulation-trained physicians with traditionally trained counterparts demonstrates equivalent or superior procedural performance during initial supervised cases.
What Device Compatibility Should We Expect?
Quality simulators accommodate multiple closure device types and manufacturers. The anatomical accuracy of the XX013D model supports training with various commercially available LAA occlusion devices, allowing institutions to practice with the specific products used in their clinical practice. The four included LAA morphologies ensure compatibility with devices designed for different anatomical configurations, from simple single-lobe appendages to complex multilobular structures requiring specialized closure approaches.
What Support Services Do Manufacturers Provide?
Reputable simulator manufacturers offer comprehensive support extending beyond initial product delivery. Trandomed provides technical assistance, replacement component availability, and guidance on optimal training program implementation. The absence of design fees for customization requests demonstrates commitment to meeting specific institutional needs. Rapid production timelines and global shipping capabilities ensure minimal delays between order placement and training program launch.
Partner with Trandomed for Advanced LAA Closure Training Solutions
Ningbo Trando 3D Medical Technology Co., Ltd brings over two decades of specialized experience in medical 3D printing technology to cardiovascular simulation. Our Left Atrial Appendage Closure Simulator represents the culmination of extensive research utilizing real human CT and MRI data, proprietary 3D printing techniques, and rigorous quality assurance processes. As a leading left atrial appendage closure simulator manufacturer, we understand the exacting standards required for effective physician training and procedural excellence.
The XX013D simulator delivers unmatched anatomical realism through its comprehensive vascular pathway reproduction, four distinct LAA morphologies, and replaceable atrial septal components. Our customization capabilities allow adaptation to your specific training objectives without additional design costs, ensuring perfect alignment with curriculum requirements. Contact jackson.chen@trandomed.com to discuss your institution's training needs, request detailed specifications, or arrange product demonstrations. Our team provides personalized consultation to help you select the optimal simulation solution that enhances physician competency, improves patient outcomes, and advances your medical education initiatives.
References
Holmes DR, Reddy VY, Turi ZG, et al. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial. Lancet. 2009;374(9689):534-542.
Di Biase L, Santangeli P, Anselmino M, et al. Does the left atrial appendage morphology correlate with the risk of stroke in patients with atrial fibrillation? Results from a multicenter study. Journal of the American College of Cardiology. 2012;60(6):531-538.
Dawson DL, Meyer J, Lee ES, Pevec WC. Training with simulation improves residents' endovascular procedure skills. Journal of Vascular Surgery. 2007;45(1):149-154.
Blackburn MC, Jansen ME. A systematic review of simulation training in interventional cardiology. Catheterization and Cardiovascular Interventions. 2017;90(5):752-762.
Reddy VY, Sievert H, Halperin J, et al. Percutaneous left atrial appendage closure vs warfarin for atrial fibrillation: a randomized clinical trial. Journal of the American Medical Association. 2014;312(19):1988-1998.
Sadeghi AH, Taverne YJHJ, Bogers AJJC, Mahtab EAF. Simulation-based cardiac surgical training: A systematic review and future directions. European Journal of Cardio-Thoracic Surgery. 2019;56(4):609-619.
_1736216292718.webp)
_1734507205192.webp)