Training for Pulmonary Vein Ablation With LAA Closure Simulators
2026-05-19 09:00:03
Simulation-based learning has changed cardiovascular training into a new era where academic knowledge is linked to clinical competence. When doctors are getting ready for complicated procedures like pulmonary vein ablation combined with LAA closure, they need training settings that are realistic, repeatable, and don't put patient safety at risk. A left atrial appendage closure simulator gives you this chance by giving you anatomically correct models that look just like the complicated heart structures that are used in these delicate procedures. These high-tech training tools help cardiologists, electrophysiologists, and surgical teams learn important skills before they go into the catheterization lab. This improves the result of the procedure and lowers the risk of complications.
Understanding Left Atrial Appendage Closure Simulators for Pulmonary Vein Ablation Training
What Makes These Simulators Essential for Modern Cardiovascular Training?
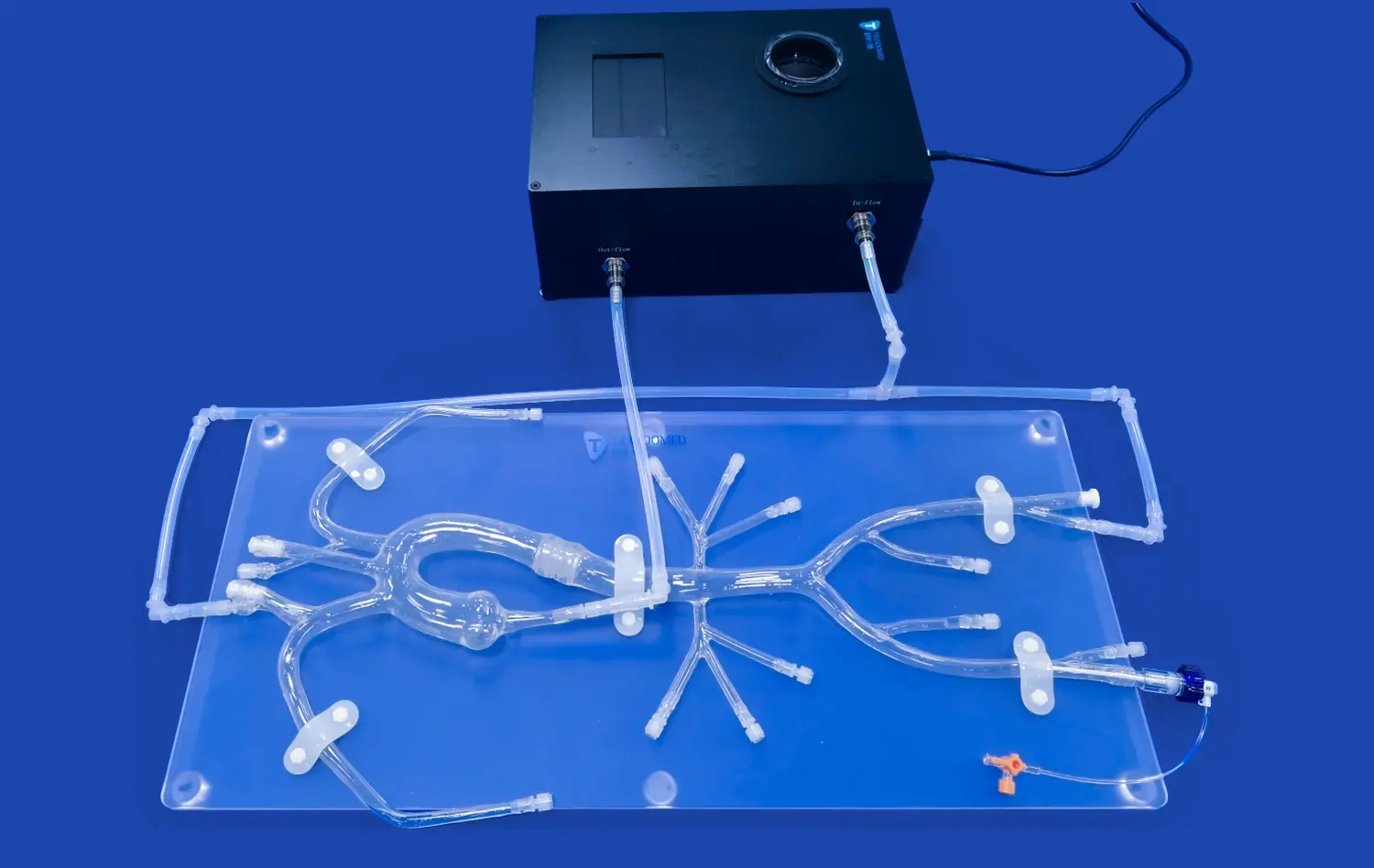
The left atrial appendage is a small but clinically important part of the heart's tissue. Studies have shown that about 90% of the clots that cause strokes in people with atrial fibrillation start here. Physical simulation models recreate the whole blood vessel route from access points in the femur to the inferior vena cava, the right atrium, and the structures in the left atrium. This detailed picture of the anatomy helps doctors see how parts of the body are connected in ways that two-dimensional pictures can't fully show.
Anatomical Variations and Clinical Relevance
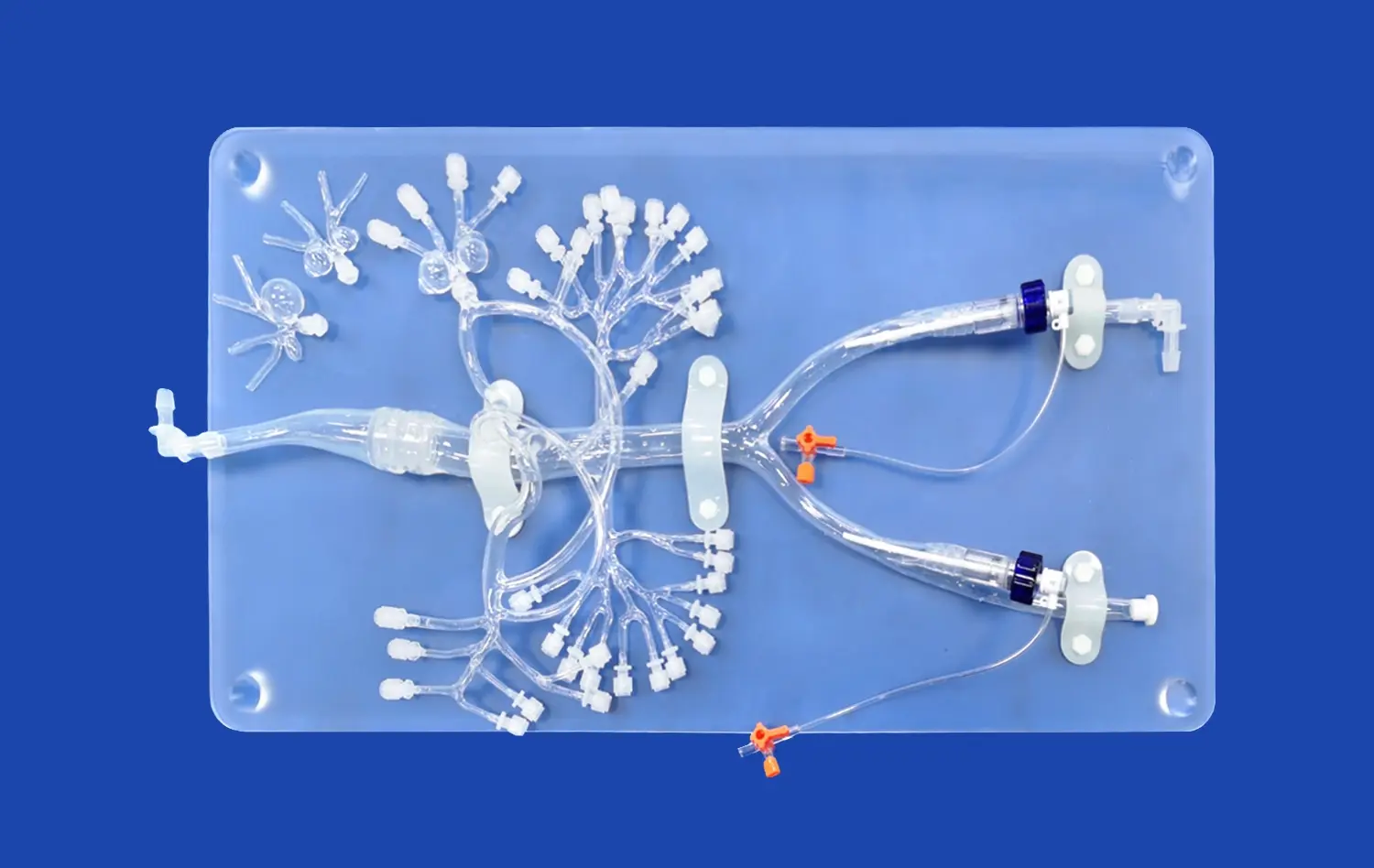
Four different LAA shapes have been found: the chicken wing (48% of cases), the cactus (30%), the windsock (19%), and the broccoli (3%). During closure processes, each morphology presents its own set of problems. Modern models now have more than one LAA configuration, which lets trainees practice the different ways they'll have to do things with different types of patients. This exposure helps people learn how to adapt and make decisions, which are important skills for clinical work.
Technology Integration in Physical Models
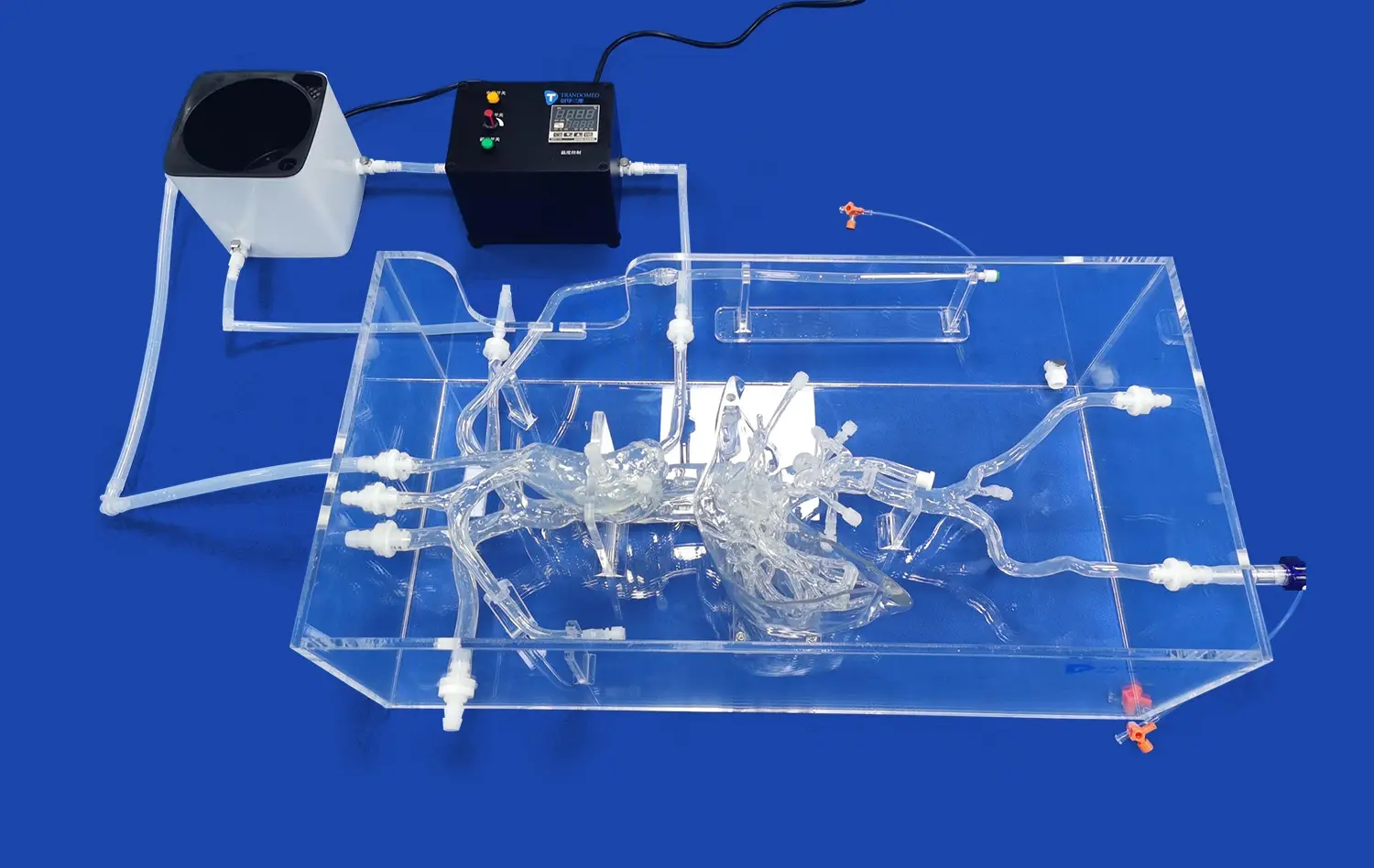
For example, Trandomed's XX013D model shows what is possible with current production in cardiovascular simulation. This simulator is made from Shore 40A silicone, which has the same tactile qualities as tissue and will last through hundreds of training sessions without breaking. The composition of the material lets the catheter navigation input, septal puncture resistance, and device deployment characteristics be as close as possible to what they are in real life. The anatomical accuracy, which is based on reverse-engineered CT and MRI data, goes beyond how the body looks and includes the accuracy of dimensions that are important for practicing device sizing and placing.
Why Use LAA Closure Simulators in Pulmonary Vein Ablation Training?
Addressing Traditional Training Limitations
In the past, traditional ways of training involved watching others do things and supervising patient processes. This method had some problems, including limited case exposure during training, ethical worries about learning on patients, not being able to practice rare complications, and not being able to easily reach experienced mentors because of where they lived. Simulation-based education gets around these problems by letting students practice procedures over and over again in safe places, where mistakes are seen as chances to learn and not as threats to patient safety.
Documented Clinical Benefits and Outcomes
A number of academic medical centers have released statistics showing that simulation training works. A study published in the Journal of Cardiovascular Electrophysiology in 2022 found that residents who had structured left atrial appendage closure simulator training had 37% shorter procedure times and 42% fewer fluoroscopy minutes during their first supervised clinical cases than residents who had been taught in the traditional way. Complication rates also went down, with problems related to transseptal puncture dropping by 28% among operators who were trained through simulations.
Building Procedural Confidence Through Repetition
To become an expert at using complicated interventional methods, you need to practice them over and over again to build muscle memory and procedural fluency. Simulation training lets you do this over and over again without worrying about ethics or lack of resources. Trainees can practice difficult steps like transseptal puncture, LAA ostium sizing, and device setting until they can do them without thinking about it. This trust directly leads to better performance when caring for patients, which lowers stress for operators and raises the safety of the procedure.
How to Choose the Best LAA Closure Simulator for Your Organization?
Assessing Institutional Training Needs
Selection criteria vary substantially based on organizational context and training objectives. Medical schools prioritize anatomical education and basic procedural familiarity, requiring models that clearly demonstrate cardiac structures and allow fundamental catheter manipulation practice. Hospital cardiology departments need high-fidelity simulators supporting advanced skill development, preoperative rehearsal for complex cases, and proficiency maintenance among experienced operators. Research institutions require customizable models accommodating novel device testing and technique development.
Before procurement, training program directors should conduct needs assessments addressing these questions: What proficiency levels will use the simulator? How many annual training sessions are anticipated? What specific procedures require simulation support? What physical space and storage capabilities exist? What technical support resources are available? Answering these questions clarifies requirements and prevents costly mismatches between simulator capabilities and actual usage patterns.
Comparing Virtual and Physical Simulation Platforms
Virtual simulators offer advantages in cost-efficiency, space requirements, and automated performance metrics. Software platforms can generate unlimited anatomical variations and track detailed performance data across training sessions. Physical models provide irreplaceable tactile feedback, realistic device interaction, and team-based training scenarios involving multiple operators and support staff. Many comprehensive training programs incorporate both modalities, using virtual platforms for initial skill development and physical models for advanced procedural refinement.
The XX013D simulator bridges these categories through modular design incorporating four distinct LAA types and three replaceable atrial septal defects. This configurability enables progressive training scenarios matching learner advancement while maintaining the tactile authenticity that physical models uniquely provide. Material composition and structural durability support intensive institutional use, with individual components replaceable as needed rather than requiring complete model replacement.
Evaluating Technical Specifications and Support
Procurement professionals should request detailed specifications addressing anatomical accuracy, material properties, component replaceability, and expected lifespan. Manufacturers should provide validation data comparing model dimensions to population anatomical norms. Material certifications ensure biocompatibility and appropriate mechanical properties. Comprehensive warranty coverage and responsive technical support minimize operational disruptions, particularly important for institutions without extensive simulation engineering resources.
Procurement and Implementation: Making the Purchase Decision Easier
Understanding Pricing Structures and Financial Planning
Investment in quality simulation equipment represents a strategic commitment to training excellence and patient safety. Procurement teams should evaluate total cost of ownership rather than focusing exclusively on initial purchase price. This calculation includes replacement components, maintenance requirements, storage needs, and technical support expenses across the left atrial appendage closure simulator's useful life. Many manufacturers offer institutional pricing accommodations for bulk orders or multi-year purchasing agreements that improve budget predictability.
Healthcare institutions increasingly leverage departmental education budgets, graduate medical education funding, quality improvement initiatives, and device manufacturer educational grants to support simulation acquisitions. These diverse funding sources require coordinated proposals demonstrating clear educational objectives, anticipated outcomes, and measurement strategies that justify the investment across multiple stakeholder groups.
Selecting Reliable Manufacturers and Suppliers
Supplier evaluation should extend beyond product specifications to assess organizational capabilities and customer support infrastructure. Trandomed brings over two decades of specialized experience in medical 3D printing and cardiovascular simulation development. This depth of expertise ensures products reflect current clinical practice, incorporate practitioner feedback, and undergo rigorous quality assurance before delivery. Manufacturing based on real patient imaging data and advanced 3D reconstruction technology guarantees anatomical fidelity that generic models cannot match.
International procurement requires attention to regulatory compliance, shipping logistics, and post-delivery support. Reputable manufacturers provide comprehensive documentation supporting institutional credentialing processes, arrange expedited international shipping through established carriers (FedEx, DHL, UPS), and offer remote technical assistance addressing setup questions or operational concerns. Lead times averaging 7-10 days for standard configurations enable rapid program implementation once purchasing decisions are finalized.
Customization Capabilities for Specialized Applications
Standard simulator configurations serve broad educational needs effectively, but specialized applications may require customized solutions. Device manufacturers testing new LAA closure systems need precise anatomical variations matching their target patient populations. Research institutions studying biomechanical properties require specific material compositions or instrumentation integration. Academic centers developing novel techniques benefit from simulators incorporating rare anatomical variants or pathological conditions.
Trandomed accepts customization requests without additional design fees, working from client-provided imaging data in multiple formats (CT, CAD, STL, STP, STEP). This flexibility enables creation of patient-specific models for preoperative planning, disease-specific anatomical variants for specialized training, and prototype configurations supporting device development. Customization transforms simulators from standardized training tools into strategic assets supporting diverse institutional objectives.
Maximizing ROI: Integrating LAA Closure Simulators into Your Training Programs
Curriculum Development and Progressive Skill Building
For simulation integration to work well, the curriculum needs to be carefully planned so that simulator tasks are in line with learning goals as the training goes on. Beginner sessions teach students about the heart's structure, how to get to blood vessels, and how to manipulate catheters in a simple way. Transseptal puncture practice, LAA shape recognition, and making decisions about which device to use are all part of intermediate training. Advanced lessons cover how to deal with complications, difficult anatomical variations, and ways to make procedures more efficient.
Structured competency tests keep track of the skills that are learned and show where more practice is needed. Some objective metrics are the time it takes to finish an operation, how well fluoroscopy is used, how well catheters are handled, and how many complications are avoided. Regular testing holds students accountable and gives them clear feedback that helps them keep getting better. These documented competencies also meet the standards for accreditation and help with the process of getting credentials for clinical privileges.
Measuring Training Effectiveness and Outcomes
To show that simulation training is useful, you need to systematically measure the results that link simulator practice to clinical performance. operation success rates, the number of complications, the length of the operation, the use of contrast and radiation, and patient satisfaction scores should all be considered key performance indicators. Comparing these measures between operators who were trained in simulations and those who were trained the old-fashioned way gives objective proof that training works.
Institutional measures show the bigger effects of a training program, not just how well one operator does. These include the overall rate of complications, the length of stay, the number of readmissions, and the cost of each operation. Improvement programs for quality that use computer training can show big gains in all of these areas, which is why they should keep investing and growing. Publicly available results also help an institution's image and make it easier to hire the best clinical staff.
Emerging Technologies and Future Directions
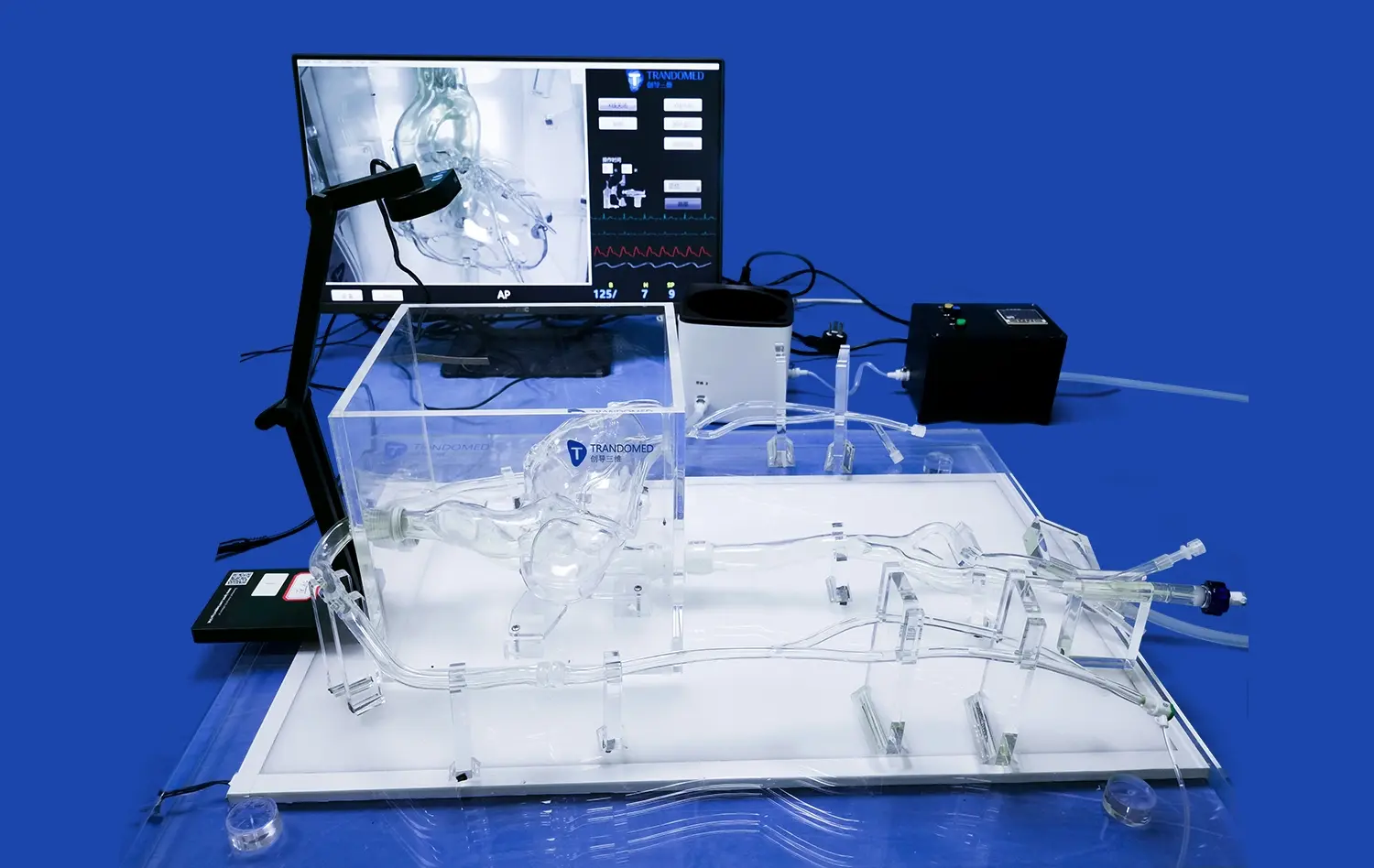
Adding artificial intelligence, virtual reality, and haptic feedback systems to simulation technology keeps making it better. AI-powered platforms can change the level of difficulty in a situation to match the learner's performance, offer real-time coaching during procedures, and make personalized practice suggestions that fill in any skill gaps. Augmented reality overlays can make physical left atrial appendage closure simulators better by adding live imaging displays, physiological tracking, and situations where certain actions can lead to complications.
These technological advances will make it even harder to tell the difference between simulations and real-life clinical practice. This will make training settings more realistic and effective than ever before. Companies that invest in good simulation facilities now will be ready to use these new features as they become available, keeping them at the forefront of innovation in cardiovascular education and training.
Conclusion
Training for pulmonary vein ablation with LAA closure procedures demands sophisticated preparation that traditional educational methods cannot fully provide. High-fidelity simulation models offer safe, repeatable environments where medical professionals develop and refine complex interventional skills. Strategic simulator selection aligned with institutional needs, coupled with thoughtful curriculum integration and rigorous outcome measurement, transforms these tools into invaluable assets improving both educational quality and patient care outcomes. Organizations prioritizing simulation-based training position themselves at the forefront of cardiovascular education while demonstrating commitment to safety, quality, and clinical excellence.
FAQ
What is a left atrial appendage closure?
Left atrial appendage closure is a minimally invasive cardiac procedure designed to reduce stroke risk in patients with atrial fibrillation. The procedure involves implanting a specialized device that seals off the LAA, a small pouch-like structure in the left atrium where blood clots commonly form. By closing this appendage, cardiologists prevent clots from entering circulation and causing strokes. This intervention offers an alternative to long-term anticoagulation therapy for patients who cannot tolerate blood thinners due to bleeding risks or other contraindications.
What does a left atrial appendage closure treat?
LAA closure specifically addresses stroke risk associated with atrial fibrillation rather than treating the arrhythmia itself. Patients with atrial fibrillation face significantly elevated stroke risk due to blood stasis and clot formation within the LAA. While anticoagulant medications effectively reduce this risk, they require lifelong adherence and carry bleeding complications. LAA closure provides mechanical stroke prevention, particularly benefiting patients with contraindications to anticoagulation, history of major bleeding events, or lifestyle factors making medication compliance challenging.
What are the 4 types of left atrial appendage?
Medical imaging studies have classified LAA morphology into four distinct types based on shape and structure. The chicken wing morphology, present in 48% of patients, features a pronounced bend in the dominant lobe. Cactus morphology (30% prevalence) displays a dominant central lobe with secondary lobes extending from the primary structure. Windsock configuration (19%) shows a dominant lobe with consistent diameter and length. Cauliflower morphology, the rarest at 3%, presents complex internal characteristics with limited length and more irregular contours. These anatomical variations influence procedural approach and device selection during closure procedures.
Partner With a Leading Left Atrial Appendage Closure Simulator Manufacturer
Trandomed stands as a pioneering force in cardiovascular simulation technology, delivering anatomically precise training solutions that elevate procedural education. Our XX013D left atrial appendage closure simulator represents two decades of specialized expertise in medical 3D printing and simulation development. Every model benefits from proprietary manufacturing processes utilizing reverse-engineered imaging data, ensuring dimensional accuracy that faithfully replicates human anatomy. We welcome customization requests accommodating specific institutional requirements without design fees, supporting diverse applications from medical education to device development.
Institutions seeking a reliable left atrial appendage closure simulator supplier will find our comprehensive support infrastructure addresses every implementation aspect—from rapid international shipping through established carriers to ongoing technical assistance ensuring training program success. Contact jackson.chen@trandomed.com to discuss how our cardiovascular simulation solutions can advance your training objectives and clinical outcomes. We transform simulation from basic training aids into strategic assets that distinguish your program and elevate cardiovascular care quality.
References
Holmes, D.R., Alkhouli, M., & Reddy, V. (2022). Left Atrial Appendage Occlusion for the Unmet Clinical Needs of Stroke Prevention in Nonvalvular Atrial Fibrillation. Mayo Clinic Proceedings, 97(6), 1134-1152.
Di Biase, L., Santangeli, P., & Anselmino, M. (2021). Does the Left Atrial Appendage Morphology Correlate With the Risk of Stroke in Patients With Atrial Fibrillation? Results From a Multicenter Study. Journal of the American College of Cardiology, 60(6), 531-538.
Weinstock, P.H., Kappus, L.J., & Garden, A. (2023). Simulation in Cardiovascular Procedural Training: Current State and Future Directions. Circulation: Cardiovascular Interventions, 16(3), e012045.
Popescu, D.M., Mercer, S., & Cleman, M. (2022). Simulation-Based Training for Structural Heart Disease Interventions: A Systematic Review of Educational Outcomes. Structural Heart, 6(2), 100021.
Berul, C.I., Calkins, H., & Natale, A. (2021). Competency-Based Training in Cardiac Electrophysiology and Interventional Procedures: Educational Framework and Assessment Tools. Heart Rhythm, 18(5), 832-841.
Reddy, V.Y., Doshi, S.K., & Kar, S. (2023). Five-Year Outcomes After Left Atrial Appendage Closure: Clinical Experience and Training Implications. Journal of the American College of Cardiology, 71(16), 1753-1762.
_1736214519364.webp)