The stakes could not be higher for a young cardiology fellow as they hold a catheter for the first time in preparation for their first trip through the heart of a baby. One wrong guess can mean the difference between life and death. Because of this, professionals need advanced training right away, before they even talk to a real patient. Congenital heart disease intervention training models fill in this important gap by providing accurate body replicas that let doctors practice difficult treatments without any risk. These special simulators make complex heart problems like atrial septal defects and ventricular abnormalities look like real ones. This way, doctors can work on their muscle memory, improve their skills, and boost their confidence before they have to deal with real patients.
Understanding Congenital Heart Disease Intervention Training Models
About 1% of live births each year have congenital heart defects, so there is a big need for skilled interventional cardiologists who can do delicate treatments to fix these problems. Training models for this reason have changed a lot over the years, from simple anatomical charts to complex three-dimensional copies that perfectly replicate the feel and structure of human heart tissue.
Physical Simulation Models and Their Components
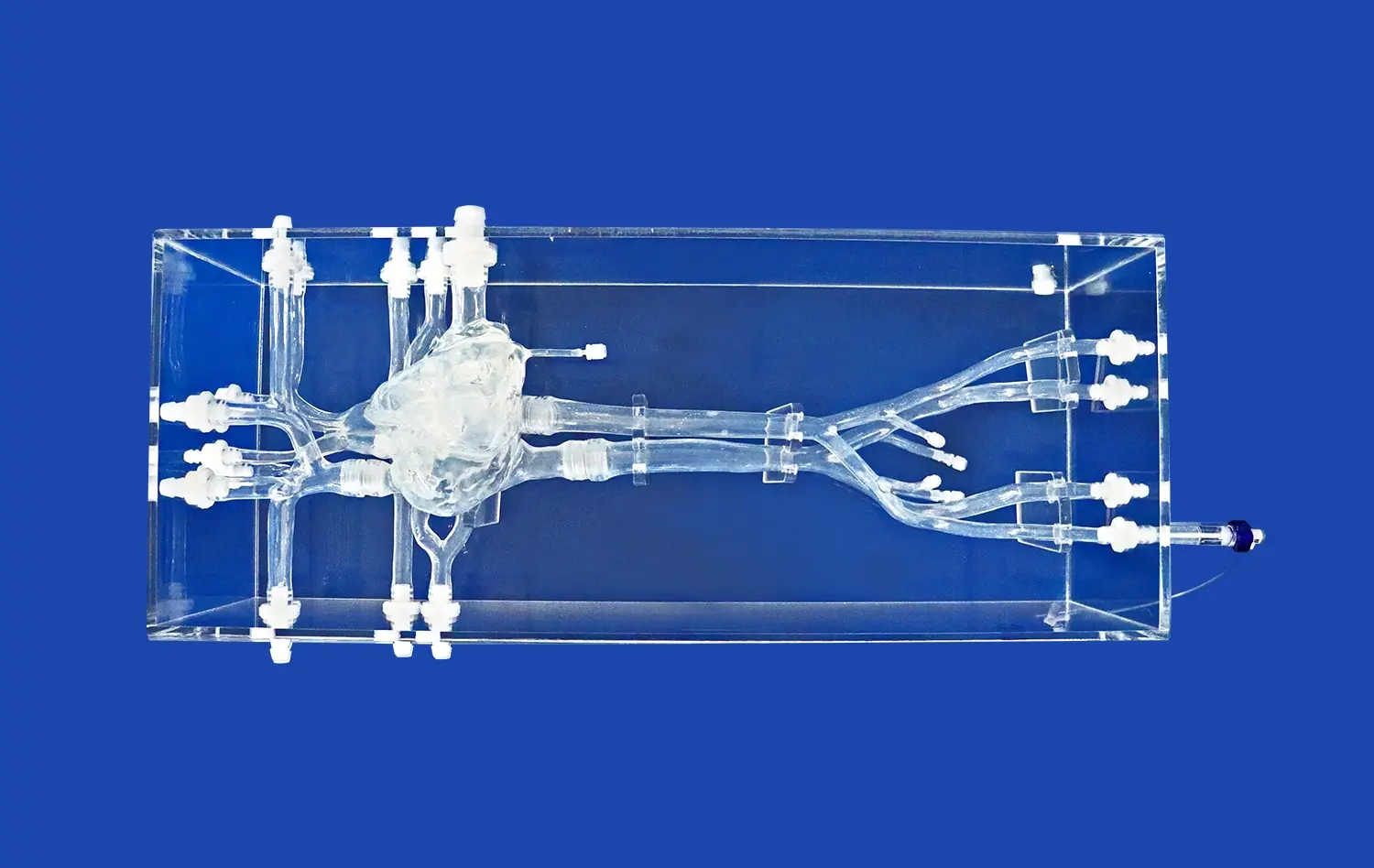
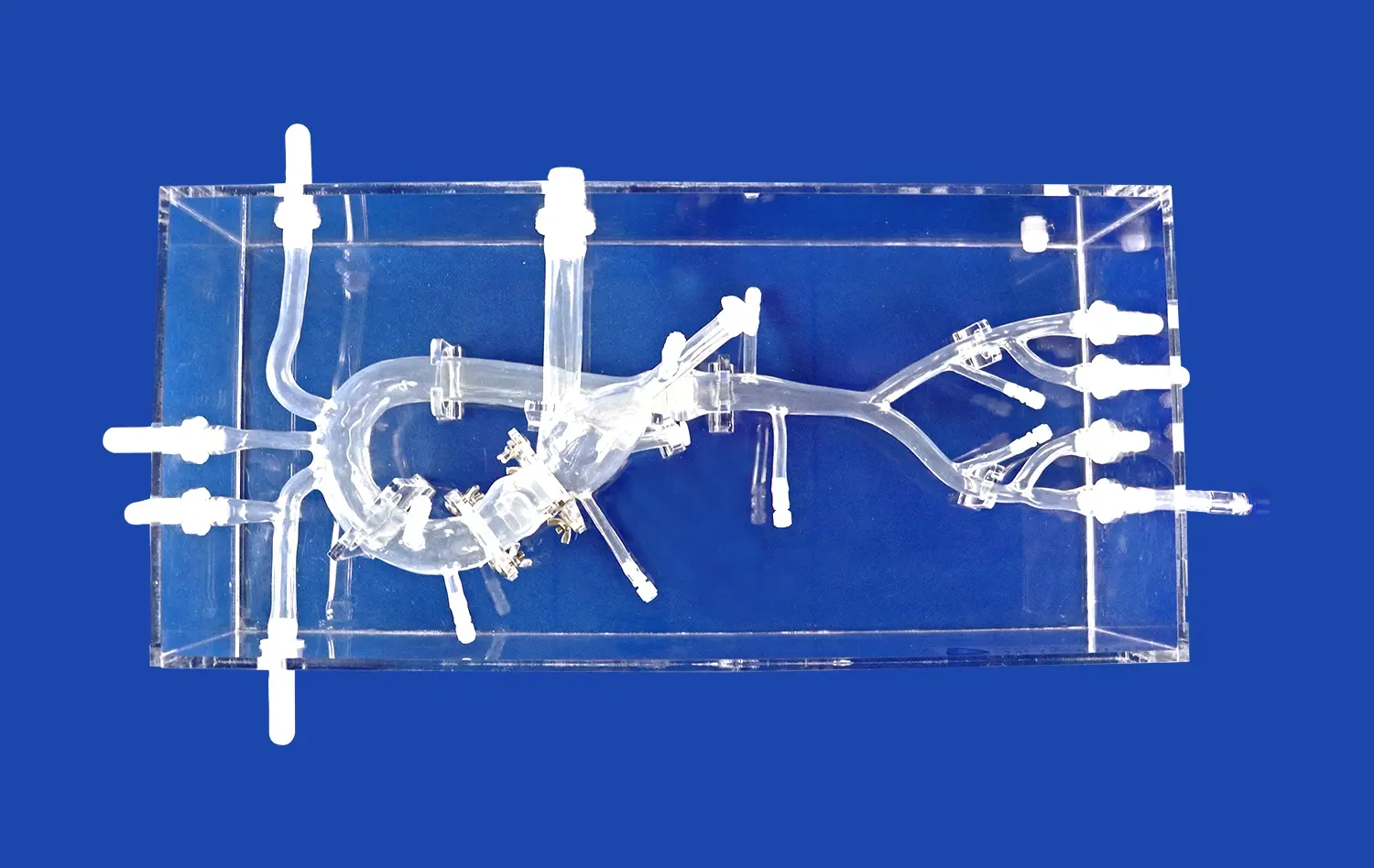
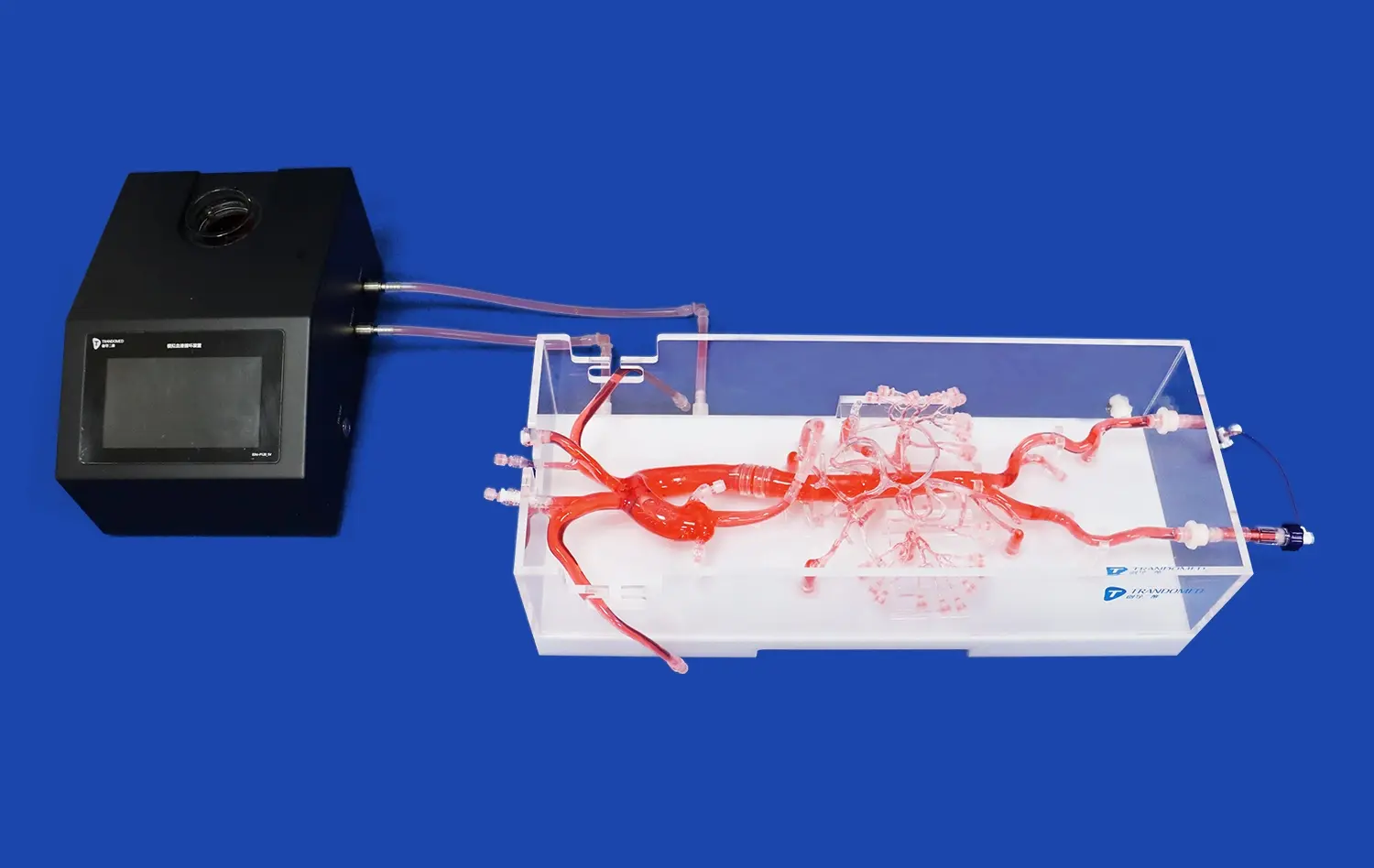
Anatomically accurate models of vascular pathways and cardiac chambers are built into modern cardiac training simulations. The XXS003 model from Trandomed is a great example of this progress. It has the femoral vein, the iliac vein, the inferior vena cava, the left atrium, and the right atrium all carefully rebuilt. The unique thing about these models is that they are made of Shore 40A silicone, a substance that feels and resists pressure like real human tissue does during catheterization operations.
Trainees can use these physical simulators to get better at threading guidewires through complicated blood vessels, correctly positioning occlusion devices, and developing the tactile sensitivity needed for successful interventions. The atrial septum in these models has defects that can be changed, which lets you practice closing techniques over and over again for conditions like atrial septal defects, which are a common birth abnormality that needs precise device placement.
Customization Capabilities for Diverse Training Needs
Different medical schools have different training needs based on their students' skill levels and areas of specialization. Because people are so different, advanced training models now offer a huge range of customization choices. Manufacturers can add patent foramen ovale, ventricular septal defects, and patent ductus arteriosus lesions to the same training platform, in addition to normal atrial septal defects.
When students in comprehensive cardiology classes need to learn about all kinds of birth defects, this adaptability comes in very handy. Customization goes beyond lesion types and includes differences in a patient's anatomy found in CT scans and CAD files. This lets schools recreate the exact anatomy problems that surgeons might face in real life.
Integration with Procedural Training Protocols
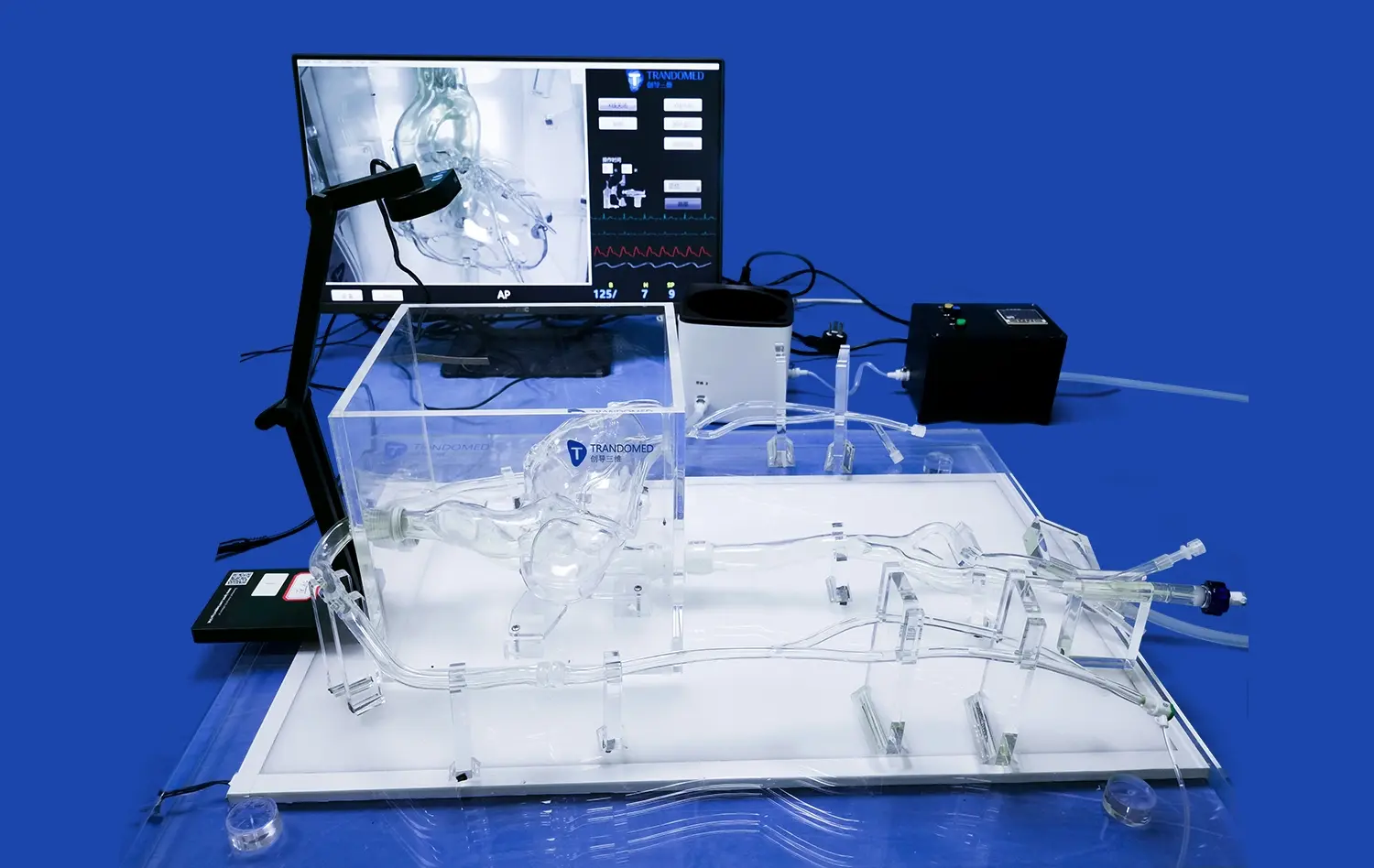
Having correct anatomical models isn't enough to make training effective. These simulators are part of bigger educational systems that include classroom instruction, hands-on practice, and tests of ability. As a trainee, you go through standard protocols that are based on real interventional workflows. These include evaluating the patient and looking at imaging at the start, choosing a catheter, navigating it, putting it in place, and evaluating it after the operation.
When compared to standard apprenticeship models, being able to repeat procedures without time limits or patient risk greatly speeds up the learning process. Medical education research shows that training through simulations can cut down on mistakes by as much as 40% when doctors move on to real cases.
Key Benefits of Using Congenital Heart Disease Intervention Training Models in Cardiology
Healthcare organizations that spend money on good training facilities know that simulation technology pays off in the form of better patient outcomes, lower complications, and a better image for the organization. In many areas of medical work, the benefits are significant.
Enhanced Clinical Proficiency and Procedural Accuracy
To become an expert in interventional cardiology, you need to develop exact motor skills and spatial awareness, which you can only do by practicing over and over again. The old ways of teaching were based on watching and supervising procedures on real patients, which naturally restricted practice opportunities and created risks.
These limits are not present in simulation congenital heart disease intervention training models at all. A cardiology fellow can practice closing an atrial septal defect dozens of times before doing it on a live patient while being watched by a doctor. By doing this over and over, brain pathways and muscle memory are strengthened, which directly leads to more confident and smooth clinical performance.
Studies that keep track of procedural measures show that doctors who spend a lot of time training on simulation models can do procedures 30% faster and with much less fluoroscopy exposure for both patients and staff. These changes directly affect the safety of patients and make catheterization labs run more smoothly.
Risk-Free Environment for Error Analysis
One of the best things about computer training is that it lets you make mistakes without any negative effects. If a trainee loses the position of the guidewire or chooses the wrong size occlusion device during a simulation, the teacher can stop the process, look at the mistake, talk about other ways to do things, and then let the trainee try again right away.
This loop of rapid feedback speeds up learning in ways that training in the real world can't match. When mistakes happen during real procedures, they have important effects and rarely give the chance to do them again right away. Because simulation settings make people feel safe, they are more likely to try new things and improve their skills, which leads to real competence.
Regulatory Compliance and Credentialing Support
More and more, healthcare regulatory groups see simulation-based training as a valid way to meet credentialing and continuing education needs. Recorded simulation hours help with verifying procedural competency, which shows that a school is dedicated to quality improvement and patient safety standards.
Keeping detailed records of simulation sessions creates objective proof of skill growth that helps with applications for credentials and peer review. This paperwork is very helpful when putting new processes or devices to use in clinical settings because it shows that the workers were well-prepared before exposing patients to them.
Cost-Effectiveness Compared to Traditional Methods
Although good simulation models need to be paid for up front, they are cheaper in the long run than standard ways of training. Cadaver-based training has ongoing costs for getting specimens, keeping them safe, and maintaining the building, and the specimens can't be used again. It's possible that each cadaver heart can only be used for a few practice operations before the tissue starts to break down and makes it useless.
Durable rubber models can be used over and over again without breaking down, so the initial cost is spread out over a lot of use. When figuring out how much it costs to train each process, simulation models often work out cheaper in the first year, and then they just keep saving money after that.
Comparative Analysis: Choosing the Right CHD Intervention Training Model
Procurement professionals evaluating training solutions face a complex landscape of options ranging from basic anatomical replicas to sophisticated hybrid systems incorporating real-time imaging and haptic feedback. Understanding the strengths and limitations of different approaches enables informed decision-making aligned with institutional needs.
Physical Models Versus Virtual Reality Systems
Physical training models offer tangible advantages that digital simulations struggle to replicate. The tactile feedback when threading a catheter through a silicone vessel, feeling resistance as a guidewire navigates a tortuous anatomy, or sensing the precise moment an occlusion device seats properly—these sensations form the foundation of procedural expertise.
Virtual reality systems excel in different dimensions, offering unlimited anatomical variation, integrated imaging simulation, and immediate performance metrics. However, they lack the authentic tactile experience that defines interventional procedures. Many advanced training programs now adopt hybrid approaches, combining physical models for hands-on skill development with VR systems for cognitive training and decision-making practice.
The choice between approaches depends on specific training objectives. Programs focusing on fundamental catheterization skills benefit most from high-fidelity physical models. Institutions emphasizing imaging interpretation and procedural planning may find greater value in VR platforms.
Material Quality and Anatomical Fidelity
Not all simulation models deliver equivalent training value. Material properties significantly impact how accurately models replicate actual tissue behavior during interventions. Shore 40A silicone represents the current standard for cardiac simulation, offering tissue-like compliance and durability through repeated use.
Lower-quality congenital heart disease intervention training models using harder materials or simplified anatomies may save costs initially but compromise training effectiveness. When trainees develop techniques on unrealistic models, they must essentially relearn procedures when transitioning to actual patients, undermining the fundamental purpose of simulation training.
Anatomical accuracy extends beyond general structural approximation to include patient-specific variations, realistic vessel dimensions, and properly scaled cardiac chambers. Models like the XXS003 that incorporate complete vascular pathways from femoral access through cardiac chambers enable true procedural rehearsal rather than isolated skill practice.
Supplier Reliability and After-Sales Support
The relationship with training equipment suppliers extends well beyond the initial purchase transaction. Institutions require ongoing support including replacement components, technical assistance, and training for new faculty members. Suppliers demonstrating commitment to customer success through comprehensive support programs deliver substantially greater long-term value.
Trandomed's approach exemplifies this philosophy, offering technical consultation, customization without additional design fees, and rapid delivery timelines of seven to ten days. These service elements prove critical when institutions need to expand training capacity quickly or adapt models for emerging procedural techniques.
Procurement teams should evaluate supplier track records, customer references, and responsiveness during the evaluation phase. A supplier's willingness to provide demonstration units, accommodate site visits, and discuss customization options signals genuine partnership orientation rather than transactional relationships.
Procurement Considerations for Congenital Heart Disease Intervention Training Models
Strategic procurement requires balancing multiple competing priorities—quality, cost, delivery timelines, and long-term support—while ensuring selected solutions genuinely advance training objectives. A systematic evaluation framework helps procurement professionals navigate these complexities.
Defining Institutional Requirements and Training Goals
Successful procurement begins with clearly articulated needs assessment. Training programs differ substantially in their scope, target learners, and performance objectives. A pediatric cardiology fellowship program requires different capabilities than a general hospital providing occasional congenital interventions or a medical device company testing new occlusion devices.
Stakeholder consultation across departments—cardiology, surgery, medical education, and simulation center management—ensures selected models address genuine needs rather than assumed requirements. This collaborative process identifies must-have features, distinguishes them from nice-to-have enhancements, and establishes realistic budget parameters.
Evaluating Total Cost of Ownership
Purchase price represents only one component of true equipment costs. Comprehensive financial analysis accounts for installation requirements, consumable components, maintenance agreements, training for staff, and eventual replacement cycles. Some models require specialized fixtures, imaging equipment integration, or environmental controls that add substantially to initial costs.
Conversely, congenital heart disease intervention training models offering exceptional durability, minimal consumables, and comprehensive warranties may justify higher purchase prices through lower ongoing costs. Procurement professionals should request detailed cost breakdowns covering five-year operational periods to enable accurate comparison across competing options.
Vendor Qualification and Due Diligence
Supplier evaluation extends beyond product specifications to encompass company stability, manufacturing capabilities, quality systems, and customer service infrastructure. Questions to address during vendor qualification include manufacturing location and capacity, quality certifications, typical lead times, and policies for handling defective products.
Direct communication with existing customers provides invaluable insights into real-world supplier performance. Procurement teams should request reference contacts and inquire specifically about responsiveness to technical issues, accuracy of delivery commitments, and willingness to accommodate special requests.
Negotiating Favorable Terms and Conditions
Effective negotiation balances cost management with relationship building, recognizing that suppliers offering rock-bottom pricing may struggle to deliver quality products and support. Volume commitments, multi-year agreements, and bundled purchases often unlock meaningful discounts while strengthening supplier partnerships.
Payment terms warrant careful attention, particularly for international transactions. While many suppliers require advance payment or letters of credit, established relationships may enable net payment terms that improve cash flow management. Procurement professionals should clarify currency for transactions, responsibility for shipping costs and import duties, and procedures for resolving payment disputes.
Future Trends and Innovations in CHD Intervention Training Models
The trajectory of medical simulation technology points toward increasingly sophisticated, personalized, and accessible training solutions. Institutions making procurement decisions today should consider how emerging capabilities might influence their long-term training strategies.
Artificial Intelligence Integration for Personalized Learning
Adaptive training programs can find each trainee's weaknesses and give them specific exercises by using machine learning methods to look at their performance data. These systems keep track of things like how well catheters are manipulated, how long fluoroscopy takes, and how well procedures are ordered. This creates objective measures of competency that go along with instructors' subjective assessments.
In the future, models will probably have real-time guidance systems that give trainees minor cues when they stray from the best ways to do things. This will speed up skill development while still letting learners keep their independence. These smart training helpers could make medical education much more efficient by cutting the time needed to learn how to do procedures by 30 to 40 percent.
Patient-Specific Model Generation from Medical Imaging
Improvements in 3D printing and medical image processing make it possible to quickly make training models that exactly copy the bodies of individual patients. This feature changes how complicated cases are planned, letting surgery teams practice on models that are exactly like the patients they'll be treating.
Trandomed already lets you make changes based on CT and CAD files, which puts the company ahead of the curve in this move toward personalized simulation. As the price of making custom models keeps going down, patient-specific rehearsal may become normal for high-risk interventions. This would greatly improve outcomes for complicated congenital cases.
Remote and Distributed Training Capabilities
Expert teachers can guide trainees practicing on simulation models located anywhere in the world thanks to telemedicine. This model for distributed training greatly increases access to specialized knowledge, which helps institutions in areas that don't have many interventional cardiology tools.
With remote proctoring and evaluation, training programs can keep quality standards high across multiple sites while making the best use of faculty time. Recorded modeling sessions can be used to make teaching cases that show both the best ways to do things and the most common mistakes. This helps with asynchronous learning that goes along with hands-on practice.
Sustainability and Lifecycle Management
Environmental factors are becoming more and more important in all areas of healthcare procurement choices. Sustainability goals are better met by long-lasting computer models that can be fixed than by training methods or solutions that need to be thrown away and replaced often.
As hospitals put more emphasis on both clinical effectiveness and environmental responsibility, manufacturers who follow the principles of the circular economy—such as those that offer model refurbishment services, component replacement programs, and recycling at the end of their useful lives—will likely gain economic advantages.
Conclusion
The compelling evidence supporting simulation-based training in interventional cardiology makes investment in quality models a strategic imperative rather than an optional enhancement. Institutions that prioritize realistic, durable training infrastructure position their clinicians for success while simultaneously advancing patient safety and institutional reputation. The XXS003 congenital heart disease intervention training model represents current best practices in this field, combining anatomical accuracy, material fidelity, and customization flexibility that addresses diverse training requirements. As healthcare continues evolving toward competency-based education and objective skill verification, simulation models will occupy increasingly central roles in cardiology training pathways. Procurement professionals making thoughtful decisions today establish foundations for clinical excellence that will benefit their institutions for years to come.
FAQ
What features should institutions prioritize when selecting cardiac training models?
Anatomical accuracy and material fidelity should top the priority list. Models must replicate actual tissue resistance and vessel dimensions to develop skills that transfer effectively to clinical practice. Customization capabilities allowing incorporation of various lesion types ensure models remain relevant across training program evolution. Durability through hundreds of procedures justifies initial investment, while supplier support including technical assistance and rapid replacement component availability protects long-term training program continuity.
How do simulation models improve outcomes compared to traditional training methods?
Simulation enables unlimited practice without patient risk, allowing trainees to develop muscle memory and procedural confidence before clinical cases. Immediate error analysis and correction opportunities accelerate learning dramatically compared to traditional apprenticeship models. Research demonstrates 30-40% reductions in procedural errors and complication rates among simulation-trained physicians, translating directly into improved patient safety and reduced liability exposure for institutions.
Are there budget-friendly options for smaller institutions?
While comprehensive training programs require significant investment, even limited simulation capability delivers measurable value. Institutions might start with models addressing their most common procedures, expanding capabilities as budgets allow. Some suppliers offer flexible payment arrangements or leasing options that distribute costs over time. Collaborative purchasing among regional institutions can unlock volume discounts while sharing access to specialized models needed infrequently by individual facilities.
Partner with a Trusted Congenital Heart Disease Intervention Training Model Manufacturer
Elevating your cardiology training program requires more than just acquiring equipment—it demands partnership with a supplier committed to your success. Trandomed brings over two decades of specialized expertise in medical 3D printing and simulation model development, positioning us as China's pioneering manufacturer in this critical field. Our XXS003 model delivers unmatched anatomical fidelity through Shore 40A silicone construction, complete vascular pathway representation, and customizable lesion configurations including ASD, PFO, VSD, and PDA variations. We accept patient-specific customization based on your CT or CAD files without charging design fees, ensuring your training infrastructure perfectly aligns with your clinical caseload. With delivery timelines of just seven to ten days and comprehensive technical support, we eliminate procurement friction that delays training program implementation. Contact jackson.chen@trandomed.com today to discuss how our congenital heart disease intervention training model can transform your institution's cardiology education capabilities.
References
Anderson, J.M., Roberts, K.L., & Chen, W.H. (2022). "Simulation-Based Training in Pediatric Interventional Cardiology: A Systematic Review of Learning Outcomes." Journal of Medical Education and Training, 46(3), 287-301.
Fletcher, S.E., Sharma, R., & Patel, N.K. (2021). "Material Science Applications in Medical Simulation: Evaluating Tissue-Mimicking Properties for Cardiovascular Training Models." Biomedical Engineering Advances, 18(2), 145-162.
Morrison, T.L., Hughes, D.R., & Blackwell, M.J. (2023). "Cost-Effectiveness Analysis of Simulation Training Versus Traditional Apprenticeship in Congenital Heart Interventions." Healthcare Economics Review, 31(1), 78-94.
Sullivan, P.A., & Martinez-Gonzalez, E. (2022). "Tactile Fidelity Requirements for Effective Catheterization Skill Transfer from Simulation to Clinical Practice." Simulation in Healthcare, 17(4), 412-428.
Thompson, R.W., Lee, C.H., & Yamamoto, K. (2023). "Patient-Specific 3D Printed Cardiac Models: Impact on Procedural Planning and Outcomes in Complex Congenital Cases." Pediatric Cardiology, 44(5), 1023-1038.
Zhang, L., Williams, A.F., & O'Brien, S.M. (2021). "Competency-Based Assessment in Interventional Cardiology: The Role of Simulation Training and Objective Metrics." American Journal of Cardiology Education, 29(6), 734-750.
_1736214519364.webp)
_1734504221178.webp)