Why LAA Closure Simulation Matters in Interventional Cardiology?
2026-05-25 09:00:03
To get good at complicated treatments in interventional cardiology, you need to be precise, have confidence, and practice over and over again. A left atrial appendage closure simulator gives doctors a safe place to practice skills they need to keep atrial fibrillation patients from having a stroke. These high-tech training tools mimic different body parts and tricky procedures, so doctors can get better at their skills before going into the catheterization lab. Simulation-based learning fills in the gaps between academic knowledge and clinical competence. This lowers the risk to patients and speeds up the learning of skills. As hospitals put patient safety and high-quality procedures at the top of their lists of priorities, cardiovascular training programs across the country need to invest in high-fidelity modeling technology.
Understanding Left Atrial Appendage Closure Simulation
What Makes LAA Closure Training Unique?
One of the most difficult minimally invasive heart treatments to do is left atrial appendage occlusion. The LAA has a lot of different shapes and sizes. Researchers have found four main types: chicken wing (48% of the time), cactus (30%), windsock (19%), and broccoli (3% of the time). This makes the procedure a lot more difficult because the devices that are used and how they are placed must be changed to fit each patient's body.
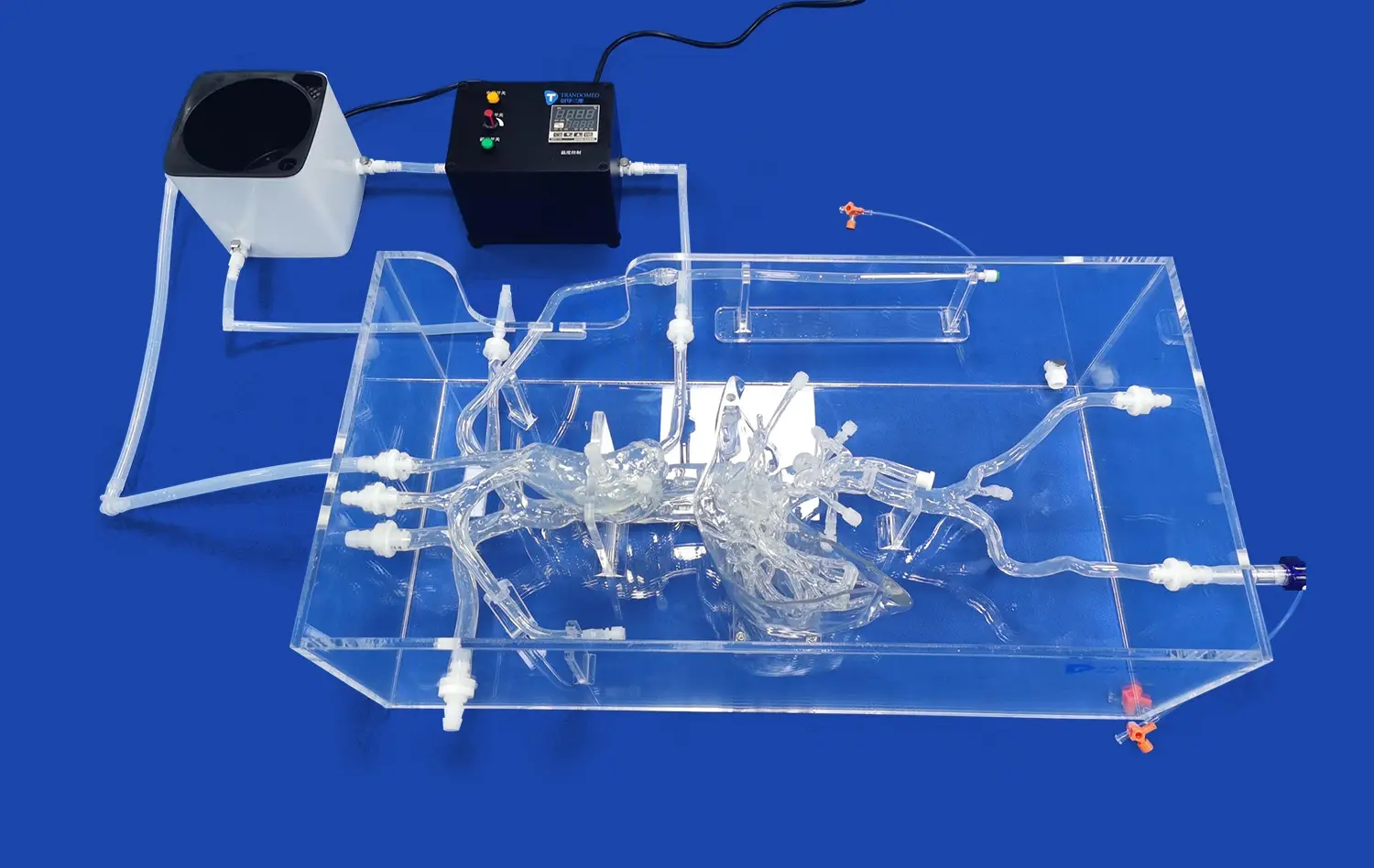
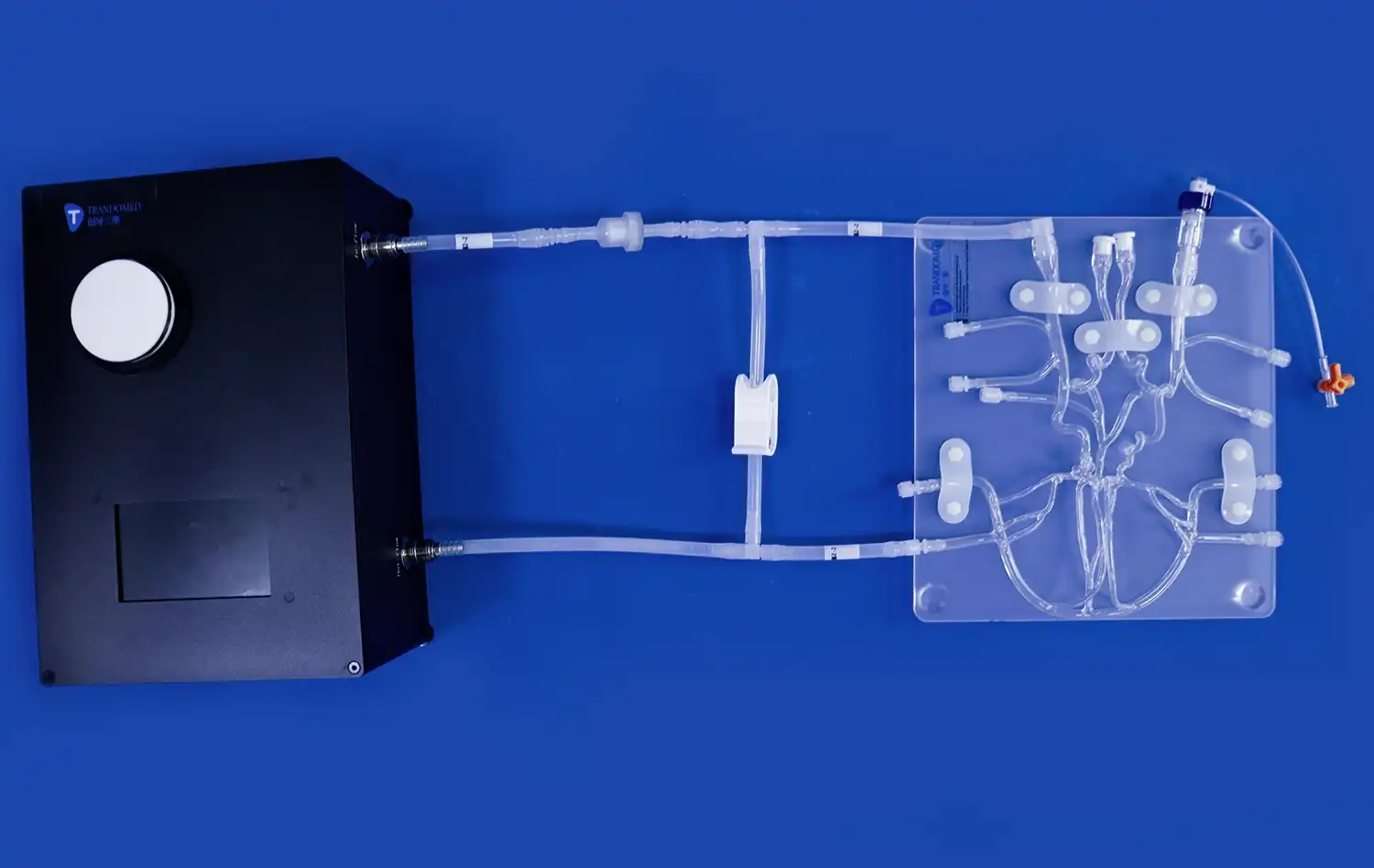
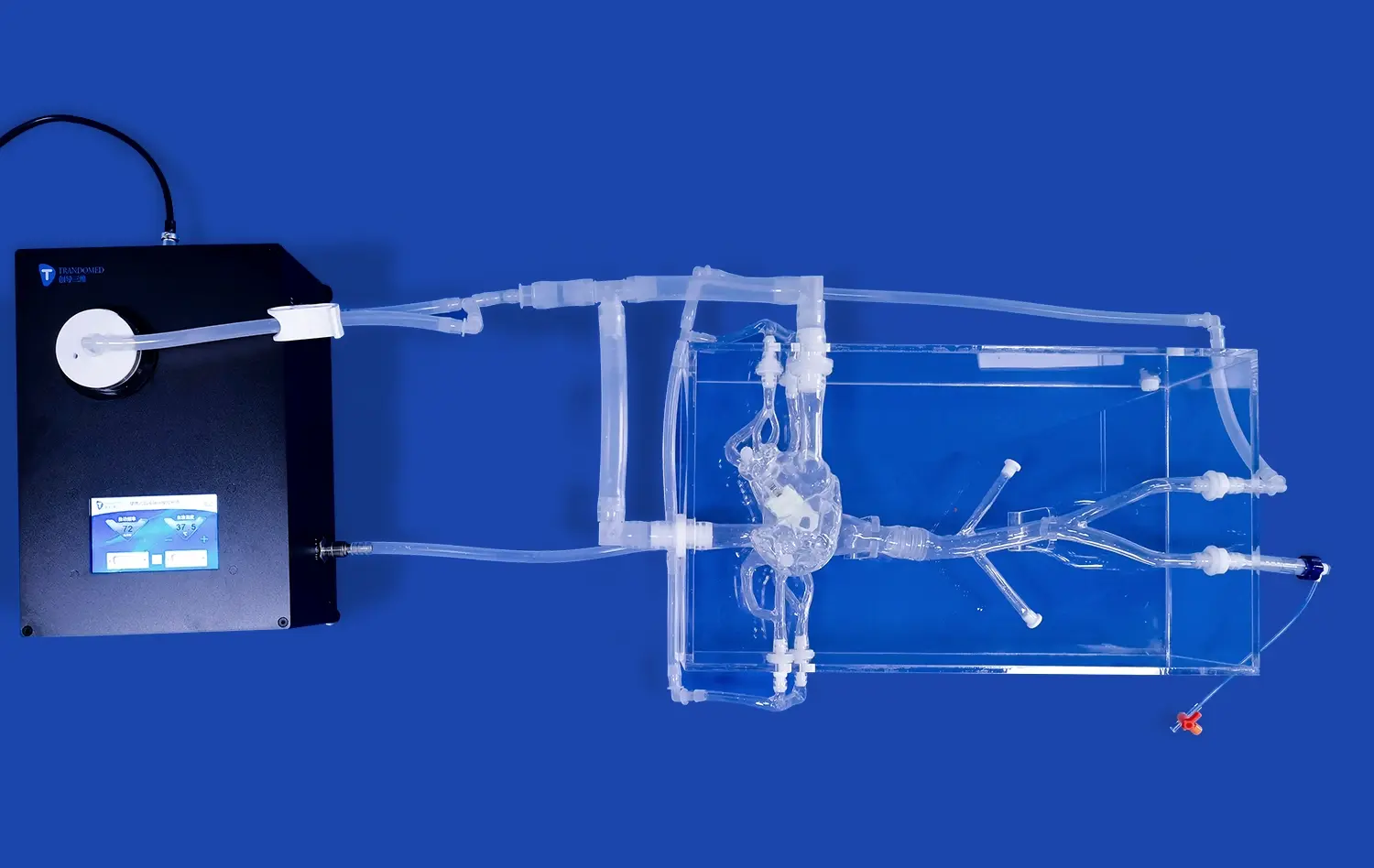
This problem is solved by physical computer models that copy real heart structures from access points in the femur through the inferior vena cava, the right atrium, and the left atrium. Modern models have replaceable parts that let trainees practice puncturing the septum, moving guidewires through complicated anatomy, and putting closure devices in place in a variety of LAA configurations. By doing this, you can improve your tactile memory and spatial awareness, which are both very important for good clinical results.
The Educational Foundation of Simulation-Based Learning
Medical school is no longer just about watching others and doing dangerous procedures on patients. Modern training methods stress focused practice in controlled environments, where mistakes are seen as chances to learn rather than threats to patient safety. Simulation technology lets cardiology fellows, interventional specialists, and electrophysiologists practice techniques over and over again until their muscles remember how to do them and their decision-making pathways become automatic.
The value in the classroom goes beyond learning technical skills. Simulation training improves how teams talk to each other, handle crises, and make the most of their process. When whole catheterization lab teams learn together using realistic models, they set rules for how to talk to each other and make sure everyone knows their job, which directly leads to better clinical performance. This all-around method of teaching procedures works on both individual skill and group performance.
Key Features and Types of Left Atrial Appendage Closure Simulators on the Market
Anatomical Fidelity and Material Science
Medical-grade silicone is used to make high-quality cardiovascular left atrial appendage closure simulators that mimic the properties of tissue that are found during real treatments. Shore 40A silicone, which is often used in advanced training models, gives feedback that feels a lot like the walls of a human blood vessel. This material's authenticity helps doctors learn how much force to use when moving catheters, crossing septa, and putting devices in place.
Anatomical precision is the most important part of a good simulation. The best training models include full vascular paths that go from the femoral access to the cardiac chambers through systemic veins. By accurately simulating the iliac vein, inferior vena cava, right atrium, interatrial septum, left atrium, and pulmonary veins, consistency is created that is similar to what happens in real life. By including four different LAA morphologies in a single training method, doctors can get a feel for the range of anatomy they see in different types of patients.
Modular Design and Procedural Versatility
The best teaching platforms have modular parts that can be put together to meet different learning goals. Atrial septal flaws that can be replaced come in different sizes, which lets doctors practice transseptal puncture many times, which is a necessary skill for getting to the LAA. These replaceable parts make simulators last longer and let schools change training settings based on the skill levels of students.
Premium modeling systems are different from basic training tools because they are more flexible. Not only do comprehensive models help with LAA occlusion practice, but they also help with related procedures like pulmonary vein ablation and complicated device navigation. This ability to do more than one procedure improves the institution's return on investment while giving trainees the chance to learn skills across all of the subspecialties of interventional cardiology.
Comparing Simulation Platforms for Institutional Procurement
When procurement teams look at training methods, they should keep a few important things in mind. Total cost of ownership is based on how long hardware lasts, since replacing parts often lowers its long-term value. High-quality silicone models can survive hundreds of procedural repetitions without breaking down, so they keep their anatomical accuracy over long training cycles.
Support infrastructure sets makers who care about their customers' success apart. Quick technical support, easy access to replacement parts, and training program consultation services all add to the total value. Partnerships with suppliers that understand educational goals and provide ongoing tools that make the best use of simulators are good for institutions.
Evaluating and Choosing the Right LAA Closure Simulator for Your Needs
Assessment Criteria for B2B Decision-Makers
To choose the right simulation technology, you need to do a thorough evaluation that fits with the goals of your school. Anatomical accuracy is the most important thing to think about—models must accurately reflect the heart structures and tissue properties that doctors see during real treatments. Hands-on testing should be done by expert interventionists who can decide how realistic the tactile elements and procedures are.
Another important factor is how easy it is to incorporate into current training programs. Instead of making things harder, simulators should make things easier in the classroom. Systems that are easy to use, don't take long to set up, and can handle multiple people at the same time are the most effective for training. Customizing anatomical features based on specific learning goals is very helpful for schools that work with a wide range of trainees.
Manufacturing Excellence and Supplier Reliability
Ningbo Trando 3D Medical Technology Co., Ltd is a leader in developing new cardiovascular modeling technology. Trandomed is the first company in China to make medical 3D printers, so every training model comes with over 20 years of specific knowledge. We start the development process by looking at a lot of real CT and MRI scans of people. We use reverse 3D modeling technology to get very accurate images of the body's details.
This dedication to quality is shown by our XX013D model. The model includes the whole blood vessel pathway, from the femoral vein to the pulmonary veins. It also has four different LAA shapes and three atrial septal defects that can be replaced. This design's flexibility lets you learn how to do foramen ovale puncture, LAA blockage, and pulmonary vein procedures all on one platform.
Real-World Performance Validation
Structured education in left atrial appendage closure simulators has been shown to improve procedural skill in medical schools, specialty hospitals, and simulation centers' clinical training programs. When trainees move from simulations to guided clinical cases, they show better spatial orientation, less time spent on fluoroscopy, and higher success rates with device deployment.
High-fidelity models are also used by device makers to create, test, and show off their products in clinical settings. Being able to show how well an implant works in a variety of body shapes speeds up the approval process for regulators and helps evidence-based marketing efforts. For biomechanical studies and protocol validation, research centers use customizable simulators that produce peer-reviewed data that moves the field forward.
Procurement Insights: Purchasing and Implementing LAA Closure Simulators
Financial Considerations and Acquisition Models
Healthcare institutions approach capital equipment purchases with rigorous fiscal discipline. Training simulator acquisition involves evaluating upfront costs against long-term educational value and patient safety improvements. Unlike consumable medical supplies, quality simulation systems deliver years of service with proper maintenance, supporting hundreds of training sessions across multiple learner cohorts.
Trandomed offers flexible procurement arrangements tailored to institutional requirements. Our T/T payment terms provide straightforward transaction processing, while our rapid production cycle ensures delivery within 7-10 days of order confirmation. This expedited timeline enables training programs to respond quickly to curriculum needs or accreditation requirements without lengthy procurement delays.
Customization Capabilities and Technical Support
One of Trandomed's distinguishing advantages lies in our comprehensive customization services. We accept client-specific modifications without charging design fees, allowing institutions to tailor simulators to precise educational objectives. Whether adjusting atrial septal defect dimensions or creating patient-specific anatomical replicas, our engineering team transforms clinical imaging data in various formats—CT, CAD, STL, STP, and STEP files—into functional training models.
This customization extends beyond initial purchase. As training programs evolve or new procedural techniques emerge, we collaborate with clients to develop enhanced components or entirely new simulation platforms. Our proprietary 3D printing technologies enable rapid prototyping and iterative refinement, ensuring training tools keep pace with clinical innovation.
Logistics and Implementation Support
Successful simulator integration requires more than product delivery. Trandomed partners with leading international carriers—FedEx, DHL, EMS, UPS, and TNT—to ensure secure, timely shipment to medical facilities throughout the United States. Our packaging protocols protect delicate anatomical components during transit, while detailed setup documentation facilitates quick deployment upon arrival.
Our after-sales commitment includes ongoing technical consultation, replacement part availability, and training program optimization guidance. We view each client relationship as a long-term partnership, invested in the success of your cardiovascular education initiatives. This comprehensive support infrastructure distinguishes Trandomed from transactional suppliers, providing confidence throughout the product lifecycle.
Future Outlook: The Evolving Role of LAA Closure Simulation in Cardiology Training
Technological Innovations Reshaping Medical Education
The convergence of artificial intelligence, augmented reality, and advanced haptics promises to revolutionize procedural simulation. Next-generation systems will incorporate real-time performance analytics, providing objective feedback on catheter manipulation, device deployment precision, and procedural efficiency. Machine learning algorithms will identify skill gaps and recommend targeted practice modules, personalizing training pathways to individual learning needs.
Augmented reality integration will overlay digital guidance onto physical left atrial appendage closure simulators, creating hybrid training environments that combine tactile authenticity with virtual instructional content. Trainees will visualize fluoroscopic perspectives, anatomical cross-sections, and device positioning simultaneously, accelerating the development of spatial reasoning skills essential for interventional cardiology.
Regulatory Evolution and Standardization
As simulation-based training demonstrates measurable improvements in clinical outcomes, regulatory bodies and professional societies increasingly incorporate competency assessment requirements into certification processes. Standardized simulation curricula ensure consistent skill development across training programs, while objective performance metrics provide transparent evaluation of procedural readiness.
This trend toward competency-based credentialing will drive sustained demand for validated training platforms. Institutions that invest proactively in high-fidelity simulation technology position themselves advantageously within evolving educational frameworks. The ability to document trainee progression through structured simulation protocols will become essential for program accreditation and graduate certification.
Global Expansion of Interventional Cardiology Access
Atrial fibrillation prevalence continues rising globally, creating expanding need for LAA closure expertise. However, geographic and economic disparities limit access to advanced procedural training in many regions. Affordable, durable simulation platforms can democratize skill development, enabling clinicians in resource-constrained settings to achieve competency levels previously accessible only at major academic centers.
Trandomed's commitment to accessible pricing and customizable solutions supports this global health equity objective. By manufacturing high-quality training tools at scale, we reduce per-unit costs while maintaining the anatomical fidelity and durability essential for effective education. This approach expands interventional cardiology capabilities worldwide, ultimately improving patient outcomes across diverse healthcare systems.
Conclusion
Simulation-based training has transitioned from supplementary educational tool to fundamental component of interventional cardiology competency development. High-fidelity models that accurately replicate LAA anatomical variations, procedural workflows, and tissue interactions enable clinicians to achieve mastery before performing live patient procedures. The XX013D simulator from Trandomed exemplifies this educational evolution, combining anatomical precision, material authenticity, and modular versatility within a comprehensive training platform. As healthcare institutions prioritize patient safety, procedural excellence, and cost-effective education, strategic investment in validated simulation technology delivers measurable returns through improved clinical outcomes and enhanced trainee confidence.
FAQ
What defines a high-quality LAA closure training model?
Premium simulation platforms exhibit several distinguishing characteristics. Anatomical accuracy derived from real human imaging data ensures trainees encounter authentic cardiovascular structures. Material properties matching human tissue provide realistic tactile feedback during catheter manipulation and device deployment. Modular design with replaceable components extends product lifespan while enabling diverse training scenarios. Manufacturing quality determines durability, with medical-grade silicone withstanding hundreds of procedural repetitions without degradation.
Can simulators replicate patient-specific anatomy?
Advanced manufacturers like Trandomed offer customization services that transform individual patient imaging data into personalized training models. By processing CT, MRI, or other digital formats, we create simulators that precisely replicate a specific patient's cardiovascular anatomy. This capability supports preoperative planning, enabling surgical teams to rehearse complex cases before entering the catheterization lab, ultimately improving procedural outcomes for challenging anatomical presentations.
How do institutions maximize training effectiveness?
Structured curricula integrating simulation with didactic education and supervised clinical experience produce optimal results. Progressive skill development—beginning with basic catheter navigation and advancing through complex device deployment scenarios—builds competence systematically. Incorporating entire catheterization lab teams in simulation sessions enhances communication and workflow coordination. Regular assessment using standardized performance metrics identifies areas requiring additional practice, personalizing training to individual needs.
Partner with Trandomed for Advanced Cardiovascular Training Solutions
Institutions seeking a trusted left atrial appendage closure simulator supplier will find Trandomed uniquely positioned to support comprehensive training objectives. Our XX013D model delivers unmatched anatomical fidelity, incorporating four distinct LAA morphologies and replaceable atrial septal defects within a complete vascular pathway from femoral access through cardiac chambers. Constructed from medical-grade Shore 40A silicone using proprietary 3D printing technology grounded in real human imaging data, this simulator provides the tactile realism and durability essential for effective procedural education. We welcome customization requests at no additional design cost, producing tailored solutions from your clinical data files within 7-10 days. Contact jackson.chen@trandomed.com today to arrange a product demonstration, discuss your specific training requirements, and discover how our two decades of medical 3D printing expertise can elevate your interventional cardiology program's educational outcomes.
References
Holmes DR, Reddy VY, Turi ZG, et al. "Percutaneous Closure of the Left Atrial Appendage versus Warfarin Therapy for Prevention of Stroke in Patients with Atrial Fibrillation: A Randomised Non-Inferiority Trial." The Lancet, vol. 374, no. 9689, 2009, pp. 534-542.
Di Biase L, Santangeli P, Anselmino M, et al. "Does the Left Atrial Appendage Morphology Correlate with the Risk of Stroke in Patients with Atrial Fibrillation?" Journal of the American College of Cardiology, vol. 60, no. 6, 2012, pp. 531-538.
Steffel J, Collins R, Antz M, et al. "European Heart Rhythm Association Practical Guide on the Use of Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation." Europace, vol. 23, no. 10, 2021, pp. 1612-1676.
Zhan Y, Soman S, Fong KY, et al. "Educational Impact of Simulation-Based Training on Procedural Competence in Interventional Cardiology: A Systematic Review." Catheterization and Cardiovascular Interventions, vol. 95, no. 6, 2020, pp. 1142-1151.
McGaghie WC, Issenberg SB, Cohen ER, et al. "Does Simulation-Based Medical Education with Deliberate Practice Yield Better Results than Traditional Clinical Education? A Meta-Analytic Comparative Review of the Evidence." Academic Medicine, vol. 86, no. 6, 2011, pp. 706-711.
Price J, Naik V, Boodhwani M, et al. "A Randomized Evaluation of Simulation Training on Performance of Vascular Anastomosis on a High-Fidelity In Vivo Model: The Role of Deliberate Practice." Journal of Thoracic and Cardiovascular Surgery, vol. 142, no. 3, 2011, pp. 496-503.
_1736215128474.webp)
 (SJ001D)_1734504338727.webp)
_1732866687283.webp)